

Case Report
Iatrogenic Right Ventricular Perforation Leading to Cardiac Tamponade in A Peritoneal Dialysis Patient: A Case Report
- Sultan Akbar
- Phillip Tran
- Leonard B. Goldstein *
A.T. Still University, School of Osteopathic Medicine in Arizona, Mesa, United States America.
*Corresponding Author: Leonard B. Goldstein, A.T. Still University, School of Osteopathic Medicine in Arizona, Mesa, United States America.
Citation: Akbar S, Tran P, Goldstein LB. (2026). Iatrogenic Right Ventricular Perforation Leading to Cardiac Tamponade in A Peritoneal Dialysis Patient: A Case Report, Journal of Clinical Research and Clinical Trials, BioRes Scientia Publishers. 5(2):1-5. DOI: 10.59657/2837-7184.brs.26.069
Copyright: © 2026 Leonard B. Goldstein, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 20, 2026 | Accepted: June 09, 2026 | Published: June 15, 2026
Abstract
Acute cholecystitis is a common illness that is treated definitively by a cholecystectomy. On occasion, a patient suffering from cholecystitis can encounter symptomatic bradycardia. When this becomes concerning, action must be taken to pace the heart. An example of this could be transvenous pacing. When a transvenous pacemaker is implanted, there is a small risk of perforating the right ventricle. When perforation occurs, a patient could potentially die of a cardiac tamponade, and urgent cardiac surgery is necessary. We present the case of a hemodialysis patient who presented with acute cholecystitis and began to subsequently have symptomatic bradycardia. Unfortunately, she suffered a right ventricular perforation during her transvenous pacemaker placement.
Keywords: bezold-jarisch reflex; pacemaker; perforation; conduction block
Introduction
Acute cholecystitis is a common but potentially life-threatening condition involving inflammation of the gallbladder, most often due to cystic duct obstruction by gallstones [1]. Clinical presentation commonly includes right upper quadrant or epigastric pain, fever, leukocytosis, nausea, vomiting, and a positive Murphy sign, although atypical presentations may occur in older adults and medically complex patients [1]. For patients deemed appropriate surgical candidates, early laparoscopic cholecystectomy during the initial hospitalization remains the preferred definitive approach [1,2]. The Tokyo Guidelines 2018 also emphasize severity grading and individualized management, including gallbladder drainage for patients who are poor operative candidates or too unstable for early surgery [2].
Cope’s sign was named after Sir Zachary Cope, who was the first patient reported with the cardio-biliary reflex [3]. The cardio-biliary reflex is thought to be vagally mediated and may be triggered by gallbladder distension, inflammation, or pain through autonomic vagal innervation [3,4]. Bradycardia is the most common clinical manifestation of this reflex, but reported cases have also described hypotension, ischemic-appearing electrocardiographic changes, high-grade atrioventricular block, and other rhythm disturbances in the setting of gallbladder disease [3,4]. Recognition of this entity is clinically important because the conduction abnormality may improve with treatment of the underlying biliary pathology and supportive care [4].
Temporary pacing is used to acutely treat bradycardia causing hemodynamically significant instability, including prolonged symptomatic pauses or high-grade atrioventricular block when a reversible cause is being treated or when permanent pacing decisions are pending [5]. Placement of a temporary pacemaker is therefore an important emergency and critical care intervention in selected patients with life-threatening bradyarrhythmias [6]. Transvenous pacing may provide more reliable cardiac capture and better short-term rate control than transcutaneous pacing, but it is invasive and carries procedure-related risks [6]. Reported complications of temporary transvenous pacing include lead dislodgement, vascular injury, bleeding, pneumothorax, infection, arrhythmia, cardiac perforation, and pericardial tamponade [7]. In a large national analysis, pericardial tamponade occurred in 0.6% of patients undergoing temporary transvenous pacemaker placement [7]. Right ventricular perforation by a temporary transvenous pacemaker is rare but potentially fatal and may require urgent pericardiocentesis, surgical repair, or both [8,9].
This case report presents a peritoneal dialysis patient with acute cholecystitis complicated by high-grade atrioventricular block who developed iatrogenic right ventricular perforation and cardiac tamponade after temporary transvenous pacemaker placement.
Case Presentation
The patient was a female in her 70s that presented to the emergency department accompanied by her daughter with a concern of abdominal pain. She was having worsening epigastric and right upper quadrant pain. A CT of the abdomen and pelvis without contrast showed a 5cm gallbladder stone, diverticulitis of the descending colon, and a moderate amount of free air (Figure 1). Additionally, it was noted that she was a peritoneal dialysis patient. She had her dialysis the same day, and the dialysis center did not believe there was anything unusual there and felt the fluid was normal in appearance.
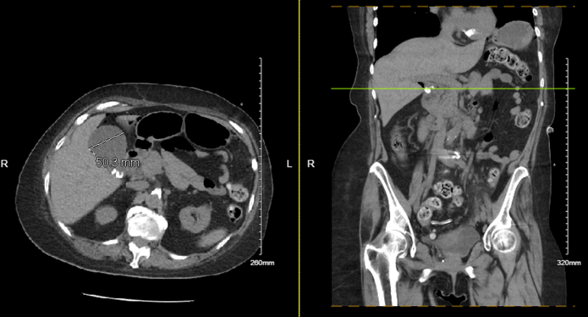
Figure 1: CT of the Abdomen and Pelvis without contrast that the patient had shown cholecystitis after appearing in the emergency room.
The patient then began to have occasional episodes of hypotension and bradycardia warranting a consult with cardiology. In the meanwhile, she began to develop a 3rd degree atrioventricular block with an escape rate of 38bpm (Figure 2). Her systolic blood pressure dropped to the 90’s. While the block spontaneously resolved, the cardiology team had her admitted to the ICU with pacer pads on and as needed dopamine. The cardiologist determined that she did not meet criteria for a permanent pacemaker.
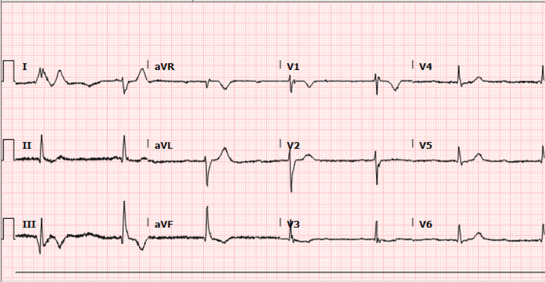
Figure 2: Electrocardiogram that the patient had in the emergency department. The rhythm was read as a normal sinus rhythm with a high-grade atrioventricular block.
In the ICU she received a consultation from a general surgeon who suspected her bradycardia was secondary to her systemic inflammatory response due to her gallbladder being infected. The belief at the time was that proceeding with a cholecystectomy would help her hemodynamics. The cardiologist seemed to believe that the patient was experiencing sick sinus syndrome in the setting of acute cholecystitis. The cardiologist then added a transvenous pacemaker to the patient’s treatment.
The patient then had a transthoracic echocardiogram which was reassuring. The left ventricular cavity size was normal with no evidence of hypertrophy. Systolic ejection velocities were normal and the left ventricular ejection fraction was 60-65%. Later that day, the plan was to proceed with a hemodialysis catheter placement. The international radiologist noted the placement to be successful and the catheter ready for immediate use.
Shortly after, the patient was having difficulty breathing, and then had a chest x-ray which showed lower lung volumes and crowding of lung markings (Figure 3). There was a left internal jugular bore catheter with a tip overlying the right atrium. There was a temporary pacemaker from the right internal jugular approach with the tip overlying the right ventricle. A follow-up transthoracic echocardiogram detected a large pericardial effusion along the right ventricular free wall, and along the right atrial wall (Figure 4). The left ventricular cavity size and systolic function was normal.
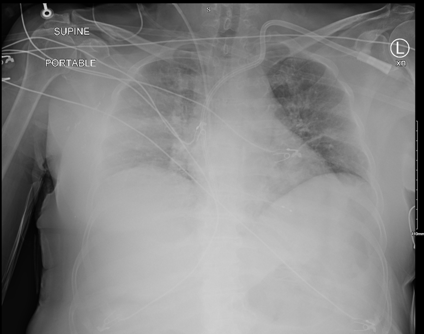
Figure 3: Chest x-ray that the patient had following her transvenous pacemaker placement.
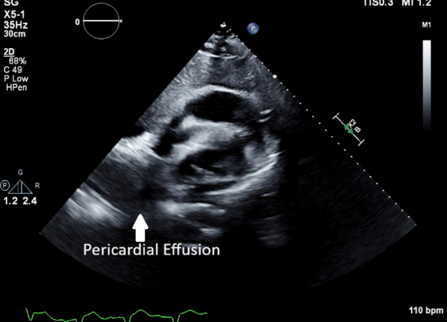
Figure 4: Transthoracic echocardiogram that the patient had that showed a large pericardial effusion.
The patient then received a pericardiocentesis due to concerns of a cardiac tamponade. This was followed by an exploratory sternotomy with right ventricular suturing (Figure 5). A repeat echocardiogram confirmed the absence of pericardial fluid. The diagnosis by the cardiology team at the time was that the patient had an iatrogenic perforation of the right ventricular wall which required an intraoperative wound closure with a successful outcome. The general surgery team reconsidered the decision to proceed with a cholecystectomy and had a percutaneous cholecystostomy placed given the patient’s condition.
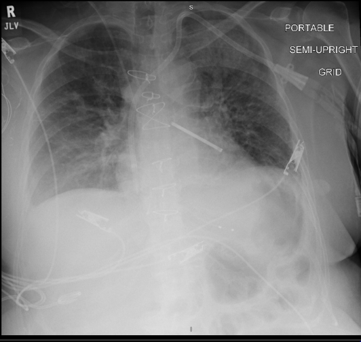
Figure 5: Chest x-ray that the patient had after her median sternotomy and left atrial appendage clipping. The tunneled left-sided dialysis catheter and right jugular temporary pacer wire were noted to be in stable condition.
When the patient had the cholecystostomy tube placed, her bedside telemetry indicated that she was less and less experiencing a third-degree atrioventricular conduction block and in sinus rhythm. The transvenous pacemaker was then removed and she remained in normal sinus rhythm with a heart rate around 70BPM.
The patient’s condition began to remarkably improve over the next few days and she was followed by nephrology to ensure the correct management of her end-stage renal disease. She also remained on empiric antibiotic treatment for sepsis. Her bedside telemetry persistently indicated that she was in sinus rhythm and she was able to be discharged.
Discussion
To start, the patient presented with a cardiac conduction abnormality in the setting of acute cholecystitis. One can speculate that this could have been an acute physiological response to the acute cholecystitis which would have potentially resolved following an emergent cholecystectomy. The Cope’s Sign is a potential etiology for what the patient was experiencing and could have been treated for using less-invasive means. Additionally, it must be noted that a transvenous pacemaker was placed as the next step in management for this case. A percutaneous pacemaker could have been used with a less likelihood of complication, but this would have to be balanced out with its lesser efficacy. What would have been the correct next step in this scenario is an incredibly subjective matter. To continue, the transvenous pacemaker placement procedure brings with it the risk of perforation. The perforation that occurred in this case could have been due to either technique or weak myocardial tissue. The patient in this case did not have any past medical history consistent with degenerative disease or heart failure, so weak myocardial tissue is an etiology that unfortunately could not have been anticipated. There are so many unknowns in this situation that it is difficult to understand what is the underlying cause for both the conduction block and the perforation.
Conclusion
Acute cholecystitis is a common complaint in a patient presenting to the emergency department. When a patient then suddenly presents with a conduction block, it is important to keep the Cope’s sign in mind when contemplating the patient’s diagnosis. Significant considerations must be made when deciding to place a transvenous pacemaker in a patient experiencing a self-resolving reflex. Further research is necessary to better formulate protocols for the usage and placement of transvenous pacemakers to prevent adverse events, because a perforation could cause a patient to experience a great amount of pain and suffering. Physicians of all specialties must be informed of the potential risks of a transvenous pacemaker placement and exercise caution in ordering them.
Statement of Informed Consent
Informed consent was obtained from the patient that was presented in the case report.
References
- Jones, M. W., Santos, G., Patel, P. J., O'Rourke, M. C., Carroll, C. (2025). Acute Cholecystitis (Nursing). In StatPearls [Internet]. StatPearls Publishing.
Publisher | Google Scholor - Yan, Y., Hua, Y., Yuan, W., Zhu, X., Du, Y., et al. (2023). Utility of Tokyo Guidelines 2018 in Early Laparoscopic Cholecystectomy for Mild and Moderate Acute Calculus Cholecystitis: A Retrospective Cohort Study. Frontiers in Surgery, 9:1022258.
Publisher | Google Scholor - Ola, R. K., Sahu, I., Ruhela, M., Bhargava, S. (2020). Cope's Sign: A Lesson for Novice Physicians. Journal of Family Medicine and Primary Care, 9(10):5375-5377.
Publisher | Google Scholor - Rajeev, A., Vinod, A., John, G. M., Jacob, P., Ramachandran, R., et al. (2022). Impact of Pelvic Bone Anatomy on Inguinal Hernia and The Role of Radiological Pelvimetry. Cureus, 14(1).
Publisher | Google Scholor - Kusumoto, F. M., Schoenfeld, M. H., Barrett, C., Edgerton, J. R., Ellenbogen, K. A., et al. (2019). 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation, 140(8):e382-e482.
Publisher | Google Scholor - Adi, O., Fong, C. P., Tze, M. K. H., Ahmad, A. H., Panebianco, N., et al. (2023). Transesophageal Echocardiography (TEE)-Guided Transvenous Pacing (TVP) in Emergency Department. The Ultrasound Journal, 15(1):35.
Publisher | Google Scholor - Metkus, T. S., Schulman, S. P., Marine, J. E., Eid, S. M. (2019). Complications and Outcomes of Temporary Transvenous Pacing: An Analysis of> 360,000 Patients from The National Inpatient Sample. Chest, 155(4):749-757.
Publisher | Google Scholor - Santana-Cabrera, L., Pérez-Acosta, G., Manzanedo-Velasco, R., Sánchez-Palacios, M. (2011). Perforation of Right Ventricle with Cardiac Tamponade Following Pacemaker Implantation. International Journal of Critical Illness and Injury Science, 1(2):169-170.
Publisher | Google Scholor - Vinther, M., Sandgaard, N. C., Risum, N., Philbert, B. T. (2024). Late Perforation of A Left Bundle Branch Area Pacing Lead Causing Ventricular Fibrillation: A Case Report. HeartRhythm Case Reports, 10(7):509-513.
Publisher | Google Scholor























