

Research Article
How Disability and Healthcare Access Are Measured: A Scoping Review of Instruments Used in Health Services Research
University Mesa, Arizona and A.T. Still University, Mesa, Arizona, United States of America.
*Corresponding Author: Leonard B. Goldstein, University Mesa, Arizona and A.T. Still University, Mesa, Arizona, United States of America.
Citation: Qadr A, Mateen Z, Jabrah A, Jamilah A, Goldstein LB, et al. (2026). How Disability and Healthcare Access Are Measured: A Scoping Review of Instruments Used in Health Services Research, Clinical Research and Reports, BioRes Scientia Publishers. 5(2):1-9. DOI: 10.59657/2995-6064.brs.26.065
Copyright: © 2026 Leonard B. Goldstein, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 27, 2026 | Accepted: June 23, 2026 | Published: June 29, 2026
Abstract
Data Sources: PubMed was searched from database inception through November 2024 using Medical Subject Headings and keywords related to disability, healthcare access, and measurement instruments. The full search strategy is provided in the Supplementary Materials. Searches were conducted between November 2023 and January 2024 and were limited to English-language publications.
Study Selection: Peer-reviewed studies examining healthcare access for patients with disabilities (PWD) or evaluating tools used to measure disability or accessibility in clinical care were eligible for inclusion. Quantitative, qualitative, mixed-methods studies, reviews, and reports aligned with the Americans with Disabilities Act definition of disability were included. Two independent reviewers screened 65 records, with disagreements resolved by consensus or a third reviewer. Twenty-four studies met final inclusion criteria.
Data Extraction: Data were extracted independently by two reviewers and included study setting, population characteristics, disability measures used, and reported barriers to healthcare access. No formal risk of bias or quality assessment was performed, consistent with the broad, descriptive scope of this review.
Data Synthesis: The 24 included studies represented diverse populations and global settings. Commonly used instruments included the Functional Independence Measure, Barthel Index, and SF-36, which primarily assess functional status or quality of life. Across studies, PWD consistently reported structural, financial, and digital barriers to care. Few instruments directly assessed accessibility or patient-reported barriers, though several studies modified or developed tools to better capture lived experience.
Conclusion: Current disability research relies heavily on functional and quality-of-life measures that inadequately capture barriers to healthcare access. Persistent structural, financial, and digital obstacles highlight the need for standardized, validated, patient-centered tools that integrate functional status with accessibility. Advancing such measures is essential to improving equity in healthcare delivery, informing policy, and guiding rehabilitation practice.
Keywords: silicone hand prosthesis; PWD; disability; ADA
Introduction
More than one billion individuals globally live with a disability, and nearly one in four adults in the United States reports a disability [1]. This population experiences disproportionately worse health care outcomes, including higher rates of chronic disease, unmet medical needs, and lower life expectancy [2,3]. These disparities are being driven not only by medical complexity, but also by structural inequities in accessing care [4-6]. Research consistently shows that people with disabilities face both interpersonal and structural barriers in health care settings [4]. These barriers present themselves in the form of inaccessible facilities and equipment, transportation, higher out-of-pocket costs, and lack of provider training in disability-competent care [5,7]. In addition to logistical barriers, people with disabilities are frequently subject to ableism and attitudinal discrimination that further erode trust and limit engagement with the health system [2,8].
Despite three decades of the Americans with Disabilities Act (ADA) having elapsed, both enforcement and compliance with accessibility standards remain suboptimal. While the ADA established a legal foundation to reduce discrimination, it has not eliminated the widespread disparities in health care access [9]. Recognition of these disparities has grown: the National Institutes of Health recently identified individuals with disabilities as a health disparity population, highlighting the importance of tackling gaps in research and clinical care [10,11].
A major step forward to increasing equity is the ability to accurately measure disability status and barriers to care. Yet, people with disabilities remain underrepresented in outcomes research, and popular access measures employed are limited in scope [12]. They concentrate on insurance or utilization without measuring daily experience of accommodation, accessibility, and environmental barriers. Similarly, instruments to assess disability vary widely, with inconsistent incorporation of functional status, participation, or patient-reported outcomes [13-15]. This lack of standardized, validated tools hinders the development of interventions and policies responsive to the needs of people with disabilities.
Accordingly, the objective of this systematic review was to identify and evaluate instruments used to measure disability status and barriers to healthcare access for people with disabilities. Specifically, we wanted to (1) characterize the tools employed in prior studies, (2) describe the barriers to care documented, and (3) highlight strengths, limitations, and future directions for measurement in this field.
Materials and Methods
This review was conducted as a systematic, descriptive synthesis of existing literature. A review protocol was developed a priori but was not registered, as the intent of this review was to broadly characterize measurement approaches rather than evaluate intervention effectiveness or pooled outcomes. The review framework, including population, exposure, and outcomes, is summarized in Table 1.
Table 1: Review Framework Including Population, Exposure, and Outcomes.
| Component | Description |
| Population (P) | People with disabilities, aligned with the Americans with Disabilities Act (ADA) definition |
| Intervention/ Exposure (I) | Use or evaluation of instruments measuring disability status, healthcare accessibility, or barriers to care |
| Comparison (C) | Not restricted; studies with or without comparison groups were eligible |
| Outcomes (O) | Identification, characterization, and evaluation of tools used to measure disability or healthcare access barriers |
Data Sources and Search Strategy
We searched PubMed from database inception through November 2024 using a combination of Medical Subject Headings (MeSH) and relevant keywords related to disability, healthcare access, and measurement tools. A summary of the search strategy is presented in Table 2, and the complete search string is provided in Supplementary Materials. Searches were conducted between November 2023 and January 2024. PubMed was selected as the sole database because of its comprehensive coverage of biomedical, rehabilitation, and health services research, and its indexing of journals most relevant to disability and accessibility scholarship. While additional databases may capture complementary literature, PubMed was deemed sufficient for this review's methodological focus.
Table 2: PubMed Search Strategy Summary.
| Database | Date Range Searched | Search Components | Filters Applied | Date Search Conducted |
| PubMed | January 1990 - November 2024 | MeSH terms and keywords related to: (1) disability (e.g., "Disabled Persons," "Learning Disabilities," disabled, disabilit*), (2) healthcare access and accessibility (e.g., "Health Services Accessibility," "Universal Design," accessible, accommodat*), and (3) measurement instruments (e.g., FIM, SF-36, Barthel Index, OHCUP, NSHD) | English language; peer-reviewed publications | November 2023 - January 2024 |
Eligibility Criteria
Studies were eligible if they included people with disabilities aligned with the ADA definition and examined healthcare access or evaluated tools designed to measure disability status or accessibility in clinical care. Quantitative, qualitative, mixed-methods studies, reviews, and reports were eligible. No restrictions were placed on study design or comparison group. Outcomes of interest included instruments used to measure disability status, accessibility, or barriers to healthcare access.
Study Selection
The final search yielded 65 records, which were independently screened by two reviewers. Studies published prior to January 1990, non-peer-reviewed articles, non-full-text publications, and non-English studies were excluded. Twenty-four articles were removed at the abstract screening stage. The remaining 41 manuscripts underwent full-text review, after which 17 were excluded for failing to meet review aims. Disagreements were resolved through discussion or consultation with a third reviewer. Twenty-four studies met final inclusion criteria.
Quality Assessment
Formal risk-of-bias or quality appraisal was not conducted, consistent with the descriptive scope of this review. As the objective was to characterize measurement approaches rather than evaluate intervention effectiveness or comparative outcomes, standardized quality assessment tools were not applied. The rationale for this approach is summarized in Table 3.
Table 3: Rationale for Measurement Approaches.
| Study Design | Risk-of-Bias Tool Applied | Rationale |
| Quantitative Studies | None | Review objective was descriptive mapping of measurement approaches rather than evaluation of intervention effectiveness |
| Qualitative Studies | None | Focus was on identification of instruments and reported barriers, not synthesis of effect sizes |
| Mixed-methods Studies | None | Heterogeneity of study designs precluded standardized quality comparison |
Final PubMed Search
("Disabled Persons"[Mesh] OR "Learning Disabilities"[Mesh] OR disabled[tw] OR disabilit*[tw] OR "learning disorder*"[tw]) AND ("Health Services Accessibility"[Mesh] OR "Universal Design"[Mesh] OR accessible[tw] OR accessibilit*[tw] OR accommodat*[tw]) AND ("Brief Pain Inventory"[tw] OR BPI[tw] OR "Functional Independence Measure"[tw] OR FIM[tw] OR RNLI[tw] OR "Reintegration to Normal Living Index"[tw] OR "SF-36"[tw] OR "SF 36"[tw] OR "36 item short form"[tw] OR "36-item short form"[tw] OR "Barthel Index"[tw] OR "OHCUP"[tw] OR "Outpatient Health Care Usability Profile"[tiab:~0] OR "National Survey on Health and Disability"[tiab:~0] OR "NSHD"[tw]).
Table 4: Study Design, Setting, and Administrative Characteristics of Included Studies.
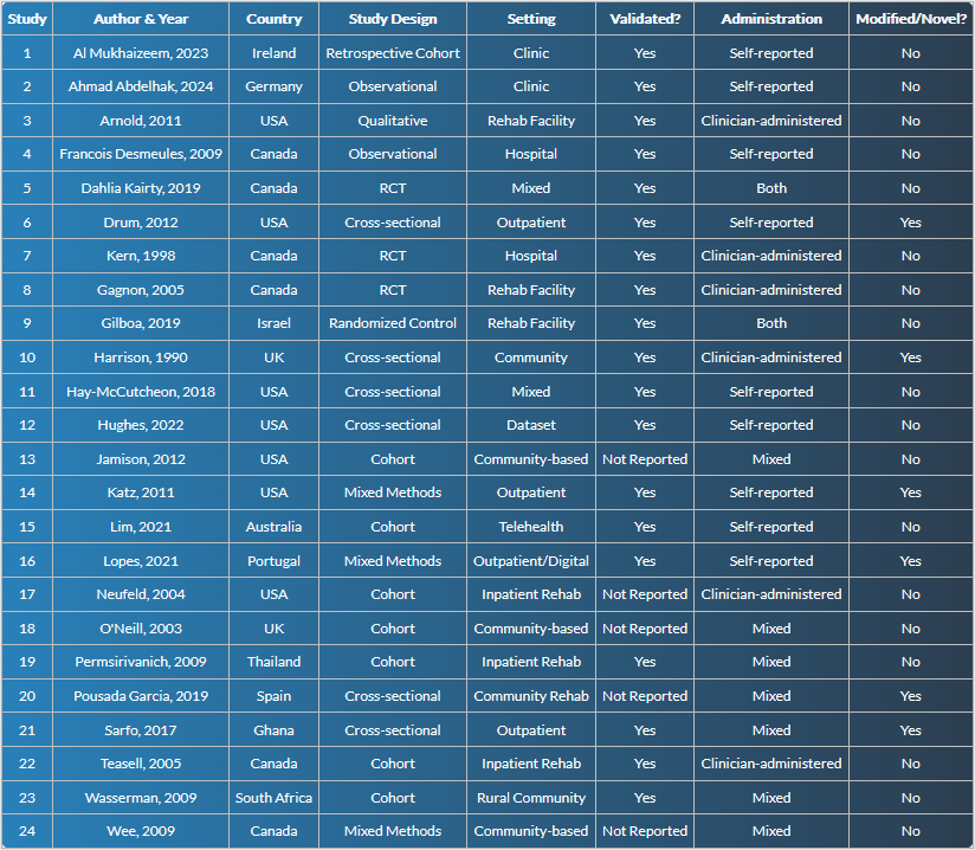
Table 5: Sociodemographic Factors Associated with Disparities in Healthcare Access Among People with Disabilities.
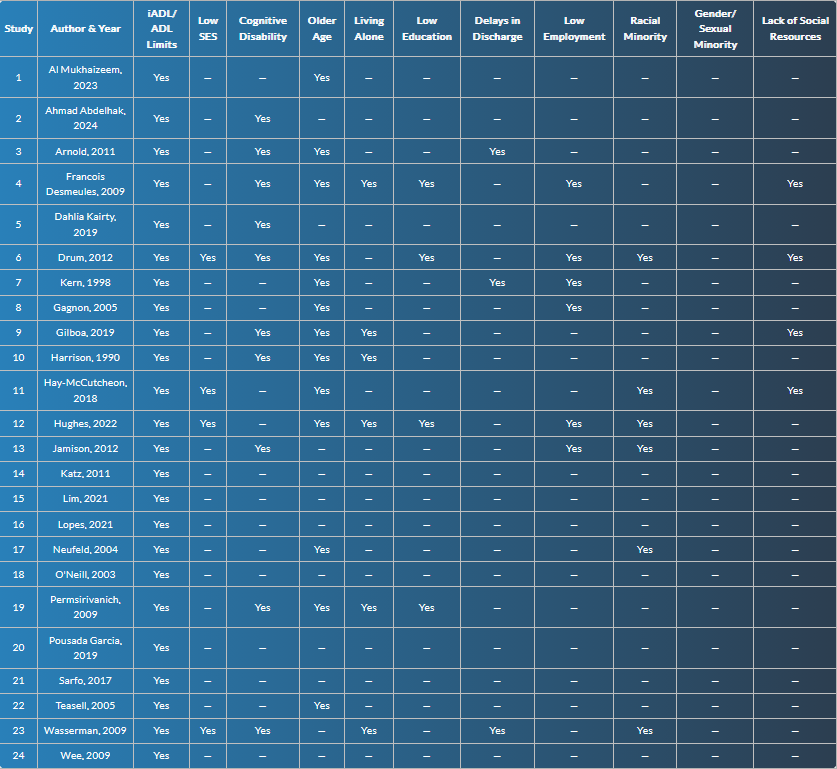
Table 6: Structural and Systemic Barriers to Healthcare Access Self-Reported by People with Disabilities.
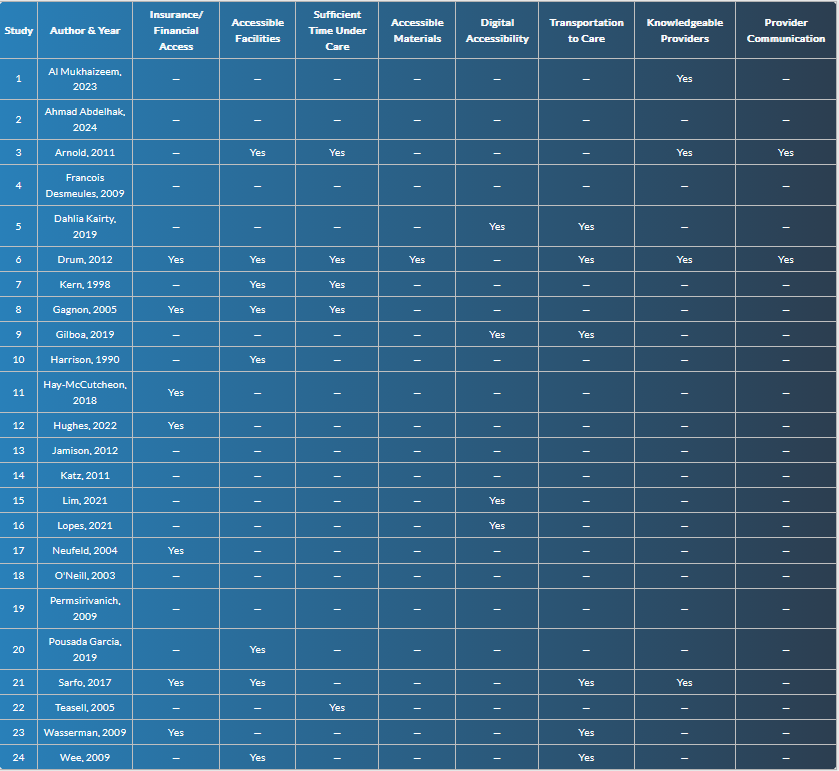
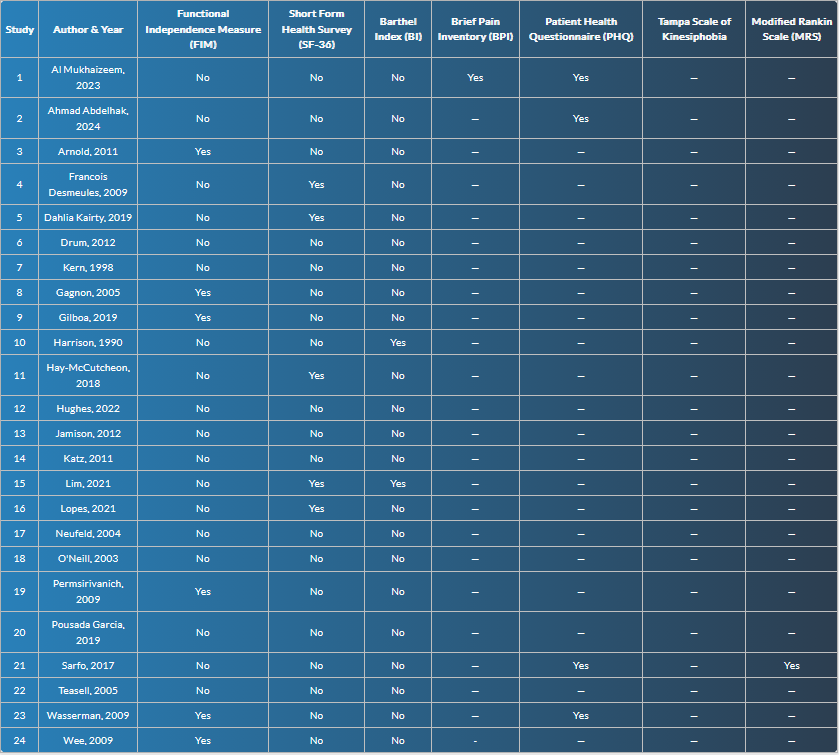
Table 7: Functional and Health Outcome Measures Used to Assess Disability Across Included Studies.
Results
Study Characteristics
The 24 included studies in this review were carried out from different parts of the world, namely the United States of America, Canada, United Kingdom, Spain, Thailand, Ghana, and South Africa. The study populations were highly varied, ranging from people with chronic pain, stroke, neuromuscular conditions, dementia, rheumatoid arthritis, hearing impairment, and traumatic brain injury. Settings varied from hospitals and outpatient clinics to residential care programs, community-based programs, with numerous studies utilizing telemedicine or mobile health apps to recruit participants. Demographic data routinely measured included age, sex, race or ethnicity, insurance, socioeconomic status, education level, and employment as reported in Tables 4-7. The variation in populations, settings, and demographics highlights the breadth of disability experiences and the complexity of healthcare access across contexts.
Measures Used to Assess Disability
Multiple instruments were used to assess disability and functional status across the included studies and are reported in Table 7. The Functional Independence Measure (FIM) was used most frequently, appearing in 8/24 studies, assessing independence in activity of daily living, transfers, locomotion, communication, and social cognition [16,17]. Short Form Health Survey (SF-36) appeared in 6/24 studies, assessing a broader range of health-related quality of life, including physical, mental, and social [13,14]. The Barthel Index (BI) was used in 4/24 studies to measure basic mobility and self-care [18]. Other tools, including Brief Pain Inventory, Reintegration to Normal Living Index, and NSHD measures, were used less frequently. Across studies, instruments primarily assessed functional ability or quality of life, with limited emphasis on patient-reported barriers to healthcare access.
Self-Reported Barriers to Healthcare Access
In the studies included, PWD self-reported a wide range of barriers to healthcare access which are depicted in Table 6. Structural barriers including inaccessible clinic settings, lack of adaptive equipment, and transportation were most commonly reported (7/24 studies).
The greatest barrier was financial constraint, with 8/24 studies indicating that patients experienced high out-of-pocket costs, inadequate insurance coverage, or limited access to in-network practitioners. Digital accessibility challenges were also reported for patients with sensory disabilities or those without smartphones or internet capabilities, limiting them to use telemedicine or mobile health apps (5/24 studies). Social environmental determinants, such as a lack of community resources, caregiver support shortages, or rural living, also restricted access to care. Although these barriers varied by setting and population, consistent patterns emerged, indicating that PWD worldwide encounter multifaceted obstacles that compromise their ability to obtain necessary health services.
Modified and Novel Tools
Several studies attempted to address gaps in traditional measurement tools by adapting or developing instruments to better capture the experiences of PWD. For example, the Valued Life Activities (VLA) questionnaire was shortened and tailored for individuals with rheumatoid arthritis to enhance its clinical relevance and utility in assessing participation in meaningful daily activities. Researchers modified the Carer Strain Index (CSI) to measure caregiver burden, home support, and rehabilitation access in stroke patients in rural Africa, highlighting the impact of environmental and social factors on patient outcomes [19]. The Outpatient Health Care Usability Profile (OHCUP) was developed with active input from patients with cognitive, mobility, and sensory disabilities to rate the usability of clinic facilities based on ADA guidelines [20]. These adaptations demonstrate the potential for more targeted measurement approaches but also reveal a need for standardized, validated tools that capture both functional status and barriers to healthcare access comprehensively.
Synthesis of Findings
Across studies, a consistent pattern emerged: commonly used disability measures emphasize impairment, independence, or general quality of life, while underrepresenting the structural, financial, and environmental barriers that shape real-world access to care. Although several studies proposed adapted or novel instruments, heterogeneity in design and limited validation restrict their generalizability [21]. Collectively, the findings highlight a persistent gap between how disability is measured and how healthcare accessibility is experienced by people with disabilities.
Discussion
This systematic review highlights the wide range of populations, settings, and measures used across studies examining healthcare access among PWD. The findings highlight three central themes. First, while many studies collected robust demographic information and spanned varied health conditions, there remains limited consistency in how disability is conceptualized and assessed. Second, the measures most frequently employed, including the FIM, BI, and SF-36, primarily capture functional status or quality of life, but do not adequately assess barriers to healthcare access. Third, across global contexts, people with disabilities consistently reported structural, financial, and digital barriers to care, pointing to a persistent and systemic inequity that extends beyond individual health systems. The reliance on functional outcome measures such as the FIM and BI reflects the longstanding biomedical framing of disability, which emphasizes impairment and physical independence [22]. While valuable for tracking rehabilitation outcomes, these tools are not designed to capture patients lived experiences of navigating healthcare systems, including inaccessible facilities, inadequate insurance coverage, or lack of provider awareness [23]. Similarly, quality-of-life tools like the SF-36 provide a broader picture of well-being but still fail to translate directly into actionable insights for improving access [24]. The absence of validated, patient-centered tools that integrate both function and access represent a significant gap in rehabilitation and health services research.
Structural barriers such as inaccessible clinics and transport are longstanding and remain central obstacles to care [20,25]. Financial access barriers like high out-of-pocket costs and narrow coverage were among the most prevalent, and reflect systemic disparities that overlap with other social determinants like race, income, and geography [2,19]. Barriers to the digital environment increase in relevance as more telemedicine emerges. For individuals with sensory impairments or limited access to technology, the digital divide risks widening existing disparities in healthcare access. Together, these barriers highlight that disability-related inequities are multifactorial and persistent across countries and healthcare systems [26,27,28]. A small number of studies in this review attempted to move beyond impairment-focused measures by modifying or developing tools to capture accessibility more directly.
The adaptation of the Valued Life Activities questionnaire for rheumatoid arthritis, the development of context-specific caregiver strain and access tools in rural Africa, and the creation of the OHCUP all reflect promising steps toward more patient-centered measurement. However, variability and lack of validation limit the generalization of these measures across multiple studies [21]. This highlights the need for standardized, validated tools able to assess accessibility in terms meaningful to patients and to providers.
The implications of these findings for rehabilitation and disability research are significant. Without tools that measure barriers to healthcare access, efforts to improve equity remain constrained. Rehabilitation clinicians may succeed in improving functional independence but fail to address the systemic and environmental factors that prevent patients from engaging fully in care. Policymakers and health systems cannot meaningfully evaluate progress toward accessibility without reliable metrics [29]. Developing validated, patient-centered measures of healthcare accessibility is therefore critical, not only for research but also for clinical practice and policy implementation.
Incorporating such tools into routine clinical practice would allow providers to identify and address barriers proactively, while also generating data to inform broader health policy [30]. Future directions should prioritize the co-design of accessibility measures with people with disabilities to ensure that patient perspectives are central [31,32]. In addition, future reviews should expand beyond PubMed, include non-English language literature, and systematically assess study quality, in order to capture a more comprehensive global picture of healthcare access for people with disabilities.
Limitations
This review has several limitations. Only one database was searched, which may have excluded relevant studies indexed elsewhere. Restricting inclusion to English-language publications may have introduced language bias, and the exclusion of gray literature may have limited the scope of findings. The absence of formal quality appraisal limits conclusions regarding the strength of evidence, and heterogeneity across study designs and outcome measures precluded direct comparison. The evolving healthcare context during the COVID-19 pandemic may also affect generalizability.
Conclusion
This systematic review demonstrates that people with disabilities face persistent and multifaceted barriers to accessing healthcare, including structural obstacles, financial constraints, and digital limitations, across diverse global contexts. While functional measures such as the FIM and BI and quality-of-life tools like the SF-36 are commonly used, they fail to capture patients lived experiences of accessibility or the specific barriers they encounter in clinical care. Adapted or novel instruments, including the Valued Life Activities questionnaire, caregiver strain measures in rural Africa, and the Outpatient Health Care Usability Profile, show promise for more patient-centered assessment, but their variability and limited validation highlight the ongoing need for standardized tools. Addressing these gaps is essential for both research and clinical practice. Validated, comprehensive measures that integrate functional status with barriers to care would allow clinicians to identify and mitigate obstacles proactively, inform policy decisions, and evaluate interventions aimed at improving equity. Co-designing these tools with people with disabilities is critical to ensure that assessment reflects lived experience and produces actionable insights. Until such instruments are widely implemented, healthcare systems risk continuing to underestimate the challenges faced by this population and falling short of providing equitable care. The findings highlight that improving healthcare access for people with disabilities requires not only attention to functional outcomes but also deliberate measurement and intervention targeting systemic and environmental barriers.
References
- National Center on Birth Defects and Developmental Disabilities. (2024). Disability Impacts All of Us Infographic. Center for Disease Control and Prevention. Disability and Health Overview.
Publisher | Google Scholor - Mahmoudi, E., Meade, M. A. (2015). Disparities in Access to Health Care Among Adults with Physical Disabilities: Analysis of A Representative National Sample for A Ten-Year Period. Disability and Health Journal, 8(2):182-190.
Publisher | Google Scholor - NCD Health Equity Framework
Publisher | Google Scholor - Iezzoni, L. I., Rao, S. R., Ressalam, J., Bolcic-Jankovic, D., Agaronnik, N. D., et al. (2022). US Physicians’ Knowledge About the Americans with Disabilities Act and Accommodation of Patients with Disability: Study Examines What Physicians Know About the Americans with Disabilities Act and What Is Done to Accommodate Patients with A Disability. Health Affairs, 41(1):96-104.
Publisher | Google Scholor - McCarthy, E. P., Ngo, L. H., Roetzheim, R. G., Chirikos, T. N., Li, D., et al. (2006). Disparities in Breast Cancer Treatment and Survival for Women with Disabilities. Annals of Internal Medicine, 145(9):637-645.
Publisher | Google Scholor - Agaronnik, N. D., Pendo, E., Campbell, E. G., Ressalam, J., Iezzoni, L. I. (2019). Knowledge of Practicing Physicians About Their Legal Obligations When Caring for Patients with Disability. Health Affairs, 38(4):545-553.
Publisher | Google Scholor - Frier, A., Barnett, F., Devine, S., Barker, R. (2018). Understanding Disability and the ‘Social Determinants of Health’: How Does Disability Affect Peoples’ Social Determinants of Health? Disability and Rehabilitation, 40(5):538-547.
Publisher | Google Scholor - Ingham, T. R., Jones, B., Perry, M., King, P. T., Baker, G., et al. (2022). The Multidimensional Impacts of Inequities for Tangata Whaikaha Maori (Indigenous Maori with Lived Experience of Disability) in Aotearoa, New Zealand. International Journal of Environmental Research and Public Health, 19(20):13558.
Publisher | Google Scholor - Scotch, R. K. (2001). American Disability Policy in The Twentieth Century. The New Disability History: American Perspectives, 375-392.
Publisher | Google Scholor - Street Jr, R. L., Haidet, P. (2011). How Well Do Doctors Know Their Patients? Factors Affecting Physician Understanding of Patients’ Health Beliefs. Journal of General Internal Medicine, 26(1):21-27.
Publisher | Google Scholor - NIH Designates People with Disabilities as A Population with Health Disparities. National Institutes of Health (NIH).
Publisher | Google Scholor - Krahn, G. L., Walker, D. K., Correa-De-Araujo, R. (2015). Persons with Disabilities as An Unrecognized Health Disparity Population. American Journal of Public Health, 105(S2):S198-S206.
Publisher | Google Scholor - Churruca, K., Pomare, C., Ellis, L. A., Long, J. C., Henderson, S. B., et al. (2021). Patient-Reported Outcome Measures (Proms): A Review of Generic and Condition-Specific Measures and A Discussion of Trends and Issues. Health Expectations, 24(4):1015-1024.
Publisher | Google Scholor - Katz, P. P., Radvanski, D. C., Allen, D., Buyske, S., Schiff, S., et al. (2011). Development and Validation of a Short Form of The Valued Life Activities Disability Questionnaire for Rheumatoid Arthritis. Arthritis Care & Research, 63(12):1664-1671.
Publisher | Google Scholor - Wasserman, S., De Villiers, L., Bryer, A. (2009). Community-Based Care of Stroke Patients in A Rural African Setting. South African Medical Journal, 99(8):579-583.
Publisher | Google Scholor - Dodds, T. A., Martin, D. P., Stolov, W. C., Deyo, R. A. (1993). A Validation of The Functional Independence Measurement and Its Performance Among Rehabilitation Inpatients. Archives of Physical Medicine and Rehabilitation, 74(5):531-536.
Publisher | Google Scholor - Iaccarino, M. A., Bhatnagar, S., Zafonte, R. (2015). Rehabilitation After Traumatic Brain Injury. Handbook of Clinical Neurology, 127:411-422.
Publisher | Google Scholor - Gresham, G. E., Phillips, T. F., Labi, M. L. (1980). ADL Status in Stroke: Relative Merits of Three Standard Indexes. Archives of Physical Medicine and Rehabilitation, 61(8):355-358.
Publisher | Google Scholor - Robinson, B. C. (1983). Validation of a Caregiver Strain Index. Journal of Gerontology, 38(3):344-348.
Publisher | Google Scholor - Drum, C. E., Horner-Johnson, W., Walsh, E. S. (2012). Construction and Validation of The Outpatient Health Care Usability Profile (OHCUP). Disability and Health Journal, 5(4):292-297.
Publisher | Google Scholor - Younas, A., Durante, A. (2023). The Logics of and Strategies to Enhance Generalization of Mixed Methods Research Findings. Methodology, 19(2):170-191.
Publisher | Google Scholor - Tedeschi, M. N., Limeri, L. B. (2024). Models of Disability as Research Frameworks in Biology Education Research. CBE-Life Sciences Education, 23(3):es8.
Publisher | Google Scholor - Williams, A. S., Moore, S. M. (2011). Universal Design of Research: Inclusion of Persons with Disabilities in Mainstream Biomedical Studies. Science Translational Medicine, 3(82):82cm12-82cm12.
Publisher | Google Scholor - Guyatt, G. (1997). Insights and Limitations from Health-Related Quality-Of-Life Research. Journal of General Internal Medicine, 12(11):720.
Publisher | Google Scholor - Hashemi, G., Wickenden, M., Bright, T., Kuper, H. (2022). Barriers to Accessing Primary Healthcare Services for People with Disabilities in Low and Middle-Income Countries, A Meta-Synthesis of Qualitative Studies. Disability and Rehabilitation, 44(8):1207-1220.
Publisher | Google Scholor - Gréaux, M., Moro, M. F., Kamenov, K., Russell, A. M., Barrett, D., et al. (2023). Health Equity for Persons with Disabilities: A Global Scoping Review on Barriers and Interventions in Healthcare Services. International Journal for Equity in Health, 22(1):236.
Publisher | Google Scholor - Padilha Clemente, K. A., da Silva, S. V., Vieira, G. I., de Bortoli, M. C., Toma, T. S., et al. (2022). Barriers to The Access of People with Disabilities to Health Services: A Scope Review. Revista de Saude Publica, 56.
Publisher | Google Scholor - Sarfo, F. S., Adamu, S., Awuah, D., Sarfo-Kantanka, O., Ovbiagele, B. (2017). Potential Role of Tele-Rehabilitation to Address Barriers to Implementation of Physical Therapy Among West African Stroke Survivors: A Cross-Sectional Survey. Journal of The Neurological Sciences, 381:203-208.
Publisher | Google Scholor - Pantaleon, L. (2019). Why Measuring Outcomes is Important in Health Care. Journal of Veterinary Internal Medicine, 33(2):356-362.
Publisher | Google Scholor - Halkides, H., James, T. G., McKee, M. M., Meade, M. A., Moran, C., et al. (2022). Spotlighting Disability in A Major Electronic Health Record: Michigan Medicine’s Disability and Accommodations Tab. JMIR Formative Research, 6(12):e38003.
Publisher | Google Scholor - Hanass-Hancock, J., Ndlovu, T., Willan, S., Zulu, N., Mhlongo, S., et al. (2025). Co-Designing the Disability Awareness Toolkit for Disability-Inclusive and Accessible Health and Post-GBV Clinical Services in South Africa. International Journal for Equity in Health, 24(1):1-16.
Publisher | Google Scholor - Morris, M. A., Sarmiento, C., Eberle, K. (2024). Documentation of Disability Status and Accommodation Needs in The Electronic Health Record: A Qualitative Study of Health Care Organizations’ Current Practices. The Joint Commission Journal on Quality and Patient Safety, 50(1):16-23.
Publisher | Google Scholor























