

Case Report
Two Rare Presentations of Primary Subcutaneous and Parietal Hydatid Cysts in Children: A Combined Case Report
- Billel Zakaria Samari *
Houari Boumediene Hospital, Sedrata, Souk Ahras, Algeria.
*Corresponding Author: Billel Zakaria Samari, Houari Boumediene Hospital, Sedrata, Souk Ahras, Algeria.
Citation: Samari BZ. (2026). Two Rare Presentations of Primary Subcutaneous and Parietal Hydatid Cysts in Children: A Combined Case Report, Journal of Surgical Case Reports and Reviews, BioRes Scientia Publishers. 5(1):1-3. DOI: 10.59657/2993-1126.brs.26.032
Copyright: © 2026 Billel Zakaria Samari, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 04, 2025 | Accepted: March 20, 2026 | Published: April 06, 2026
Abstract
Background: In contrast to adults, several pediatric studies have indicated that the lungs are more frequently involved than the liver in children. However, atypical locations such as subcutaneous tissues or the abdominal wall are extremely rare (2), posing diagnostic challenges, especially in endemic regions.
Case Presentation: We report two pediatric cases: (1) a primary subcutaneous hydatid cyst of the thigh, and (2) a primary hydatid cyst of the anterior abdominal wall. Both patients living in rural regions with frequent animal contact, presented with slowly growing and painless masses. Radiologic evaluation suggested cystic lesions without visceral involvement and negative serology. Complete surgical excision was performed in both cases, confirming hydatid disease intraoperatively. Both children recovered uneventfully.
Conclusion: These cases highlight the need for clinicians to consider hydatid cysts in the differential diagnosis of superficial or parietal masses in endemic areas.
Keywords: children; primary subcutaneous hydatid cyst; case report
Case Presentation 1
Subcutaneous Hydatid Cyst of the Thigh
A 10-year-old girl from a rural area in Eastern Algeria presented with a two-week history of a gradually enlarging, painless swelling on the anteromedial aspect of her left thigh. There was no history of trauma, fever, or weight loss. Except for frequent animal contact, her past medical history was unremarkable.
On physical examination, a 4 cm, well-circumscribed, mobile, non-tender subcutaneous mass was noted. The overlying skin was normal with no signs of inflammation. No regional lymphadenopathy was present.
Ultrasonography showed a well-defined, anechoic cystic lesion confined to the subcutaneous tissue without septations or solid components. No hepatic or abdominal hydatid cysts were detected.
Surgery was performed under general anesthesia. A careful dissection revealed a translucent pericyst and a germinative membrane characteristic of a hydatid cyst. The postoperative course was uneventful and the patient was discharged on day 02.
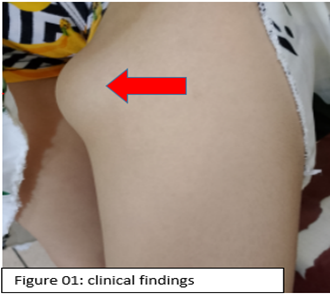
Figure 1
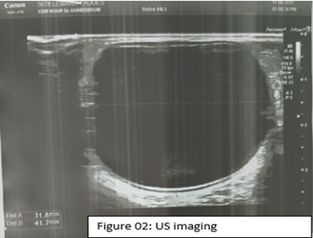
Figure 2

Figure 3
Case Presentation 2
Primary Hydatid Cyst of the Anterior Abdominal Wall
A 12-year-old boy presented with a progressive swelling in the right lower quadrant of the abdomen that had been increasing in size over approximately three months. The swelling was painless, with no history of trauma, fever, or digestive symptoms. Physical examination revealed a 6 cm, soft, cystic, non-tender mass located in the anterior abdominal wall. The mass had limited mobility and appeared attached to deeper parietal tissues. The skin over the mass was normal. Ultrasound demonstrated a well-defined cystic lesion within the abdominal wall musculature. No abdominal organ involvement was seen. Laboratory tests, including eosinophil count and liver function, were normal. Surgical exploration confirmed a hydatid cyst embedded in the muscular plane. The cyst was excised completely without rupture. Postoperative albendazole was administered. Recovery was smooth, and follow-up examinations showed no recurrence.
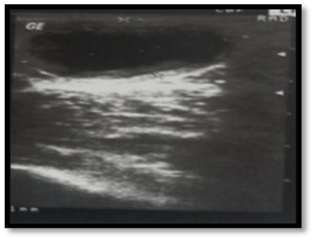
Figure 4

Figure 5
Discussion
Unlike in adults, research on children has shown that the lungs are more commonly affected than the liver. Nonetheless, occurrences in unusual areas like the subcutaneous tissues or the abdominal wall remain uncommon for both populations [1,2]. The two cases we described illustrate these unusual manifestations in the pediatric population. The pathophysiology of primary subcutaneous or parietal hydatid disease is unclear. Possible mechanisms include systemic larval dissemination bypassing hepatic and pulmonary filters or direct lymphatic spread [3]. In endemic areas, the child’s environment provides essential diagnostic clues. Both children in our report lived in rural settings and had frequent contact with dogs and livestock. Therefore, practitioners working in such regions must consider echinococcosis as a differential diagnosis whenever a child presents with a slowly enlarging, painless, well-defined mass, even when imaging and serology are inconclusive and no hepatic or pulmonary cysts were found. Missing this diagnosis may lead to inappropriate procedures, such as needle aspiration or biopsy, which carry the risk of cyst rupture or anaphylaxis [4,5]. Ultrasonography remains the first-line imaging modality [6], and complete surgical excision without rupture remains the gold standard treatment to prevent recurrence or potential anaphylactic reactions [7].
Conclusion
We reported these two cases to underscore the importance of including hydatid disease in the differential diagnosis of any superficial or parietal mass in children living in endemic regions, especially in cases of frequent animal contact. Maintaining this level of awareness can significantly improve diagnostic accuracy, avoid dangerous procedures, and ensure timely and effective treatment.
References
- Kayaalp C, Aydın C, Kaplan M, Koçer M, Ceylan M. (2024). Clinical pattern of pediatric hydatid disease: a retrospective cohort study. J Surg Med. 8(5):636-641.
Publisher | Google Scholor - Tekin R, Avcı E, Kadioglu H, et al. (2021). Pulmonary hydatid cysts in children: a single-center 20-year experience. J Pediatr Surg. 56(12):2295-2301.
Publisher | Google Scholor - Patmano, M., Çetin, D. A., Gümüş, T., Patmano, G., Yenigül, A. E. (2022). Primary soft tissue hydatid cysts. Turkish Journal of Parasitology. 46(2):145-149.
Publisher | Google Scholor - WHO Informal Working Group. (2003). International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Tropica, 85(2):253-261.
Publisher | Google Scholor - Sayek, I., Tirnaksiz, M. B., Dogan, R. (2004). Cystic hydatid disease: current trends in diagnosis and management. Surgery Today, 34(12):987-996.
Publisher | Google Scholor - García MB, et al. (2000). Primary solitary hydatid cyst in the subcutaneous tissue of the thigh. Acta Dermato-Venereologica. 80(2):160-161.
Publisher | Google Scholor - Mir MA, et al. (2017). Primary soft tissue hydatid cyst of thigh. Int J Surg Case Rep. 36:74-76.
Publisher | Google Scholor























