

Case Report
Silenced By Swelling: Navigating Anaesthesia in An Infant with Giant Oral Lymphangioma-A Case Report
- Rahul Kumar Chaudhary ID 1*
- Rojina Sedhai 1
- Satish Kumar Thakur 1
- Anuja Pokharel 1
- Kanak Khanal 1
- Rahul Mahato 2
- Hiramani Pathak 3
1 Department of Anesthesiology and Critical Care, Birat Medical College Teaching Hospital, Morang, Nepal.
2 Department of Head and Neck Surgery, Birat Medical College Teaching Hospital, Morang, Nepal.
3 Department of Pediatric Surgery, Birat Medical College Teaching Hospital, Morang, Nepal.
*Corresponding Author: Rahul Kumar Chaudhary,Department of Anesthesiology and Critical Care, Birat Medical College Teaching Hospital, Morang, Nepal.
Citation: Rahul K. Chaudhary, Sedhai R, Satish K. Thakur, Pokharel A, Khanal K, et al., (2026). Silenced By Swelling: Navigating Anaesthesia in An Infant with Giant Oral Lymphangioma-A Case Report. International Journal of Medical Case Reports and Reviews, BioRes Scientia Publishers. 6(1):1-4. DOI: 10.59657/2837-8172.brs.26.088
Copyright: © 2026 Rahul Kumar Chaudhary, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 08, 2026 | Accepted: April 22, 2026 | Published: April 29, 2026
Abstract
Background: Lymphangiomas are benign congenital malformations occurring in 1.2--2.8/1000 births, with 50% detected at birth and 90% by age 2. Most (75%) occur in the head/neck, while 15% involve the axilla. Surgical excision remains standard treatment.
Case Summary: We present a 7-month-old infant with a giant oral lymphangioma occupying nearly the entire oral cavity, extending from the mandible to clavicle and originating from the tongue base and floor of the mouth. Magnetic resonance imaging revealed a heterogeneous T2-hyperintense lesion. The mass was excised under general anaesthesia, which posed significant challenges: difficult intubation, risk of ventilation obstruction (bag-mask issues, subglottic edema), and postoperative airway compromise from oropharyngeal edema. A multidisciplinary approach with preparedness for surgical airway intervention was critical to ensuring safety.
Conclusion: This case reinforces the anaesthetic and surgical complexities of giant oral lymphangiomas in infants, emphasizing the need for meticulous perioperative planning, including contingency measures for airway emergencies.
Key clinical message
Giant oral lymphangiomas in infants demand meticulous airway planning, multidisciplinary teamwork, and readiness for tracheostomy due to high obstruction risks. Persistent post-op edema often requires prolonged ventilation or a surgical airway. Vigilant monitoring is essential throughout the perioperative period.
Keywords: lymphangioma; anaesthesia; surgical excision; tongue; tracheostomy
Introduction
Lymphangiomas are congenital benign lesions of lymphatic system occurring within the range of 1.2 to 2.8 cases out of 1000 live births [1]. About 50 percent of cases manifest themselves at birth and 90 percent of them are identified during the initial years of life, and the head and neck region is the most common site [2]. The first account of lymphangiomas was made by Redenbacher in 1828 and of tongue lymphangiomas was made by Virchow in 1854 [3]. The malformations can also be associated with Turner and Noonans syndrome and other chromosome abnormalities [4]. The peripheral malformations are due to atypical structures of the plexus in periphery of the body [5]. Major complications of such malformations are infection and increase in the size of swelling leading to obstruction and cosmetic deformity [6]. Timely diagnosis and therapy is very crucial to reduce functional, psychological and cosmetic loss [7]. Airway management of these malformation patients is always a challenge. Problems associated with it are poor visibility of the airway, extrinsic and intrinsic compression with distortion, haemorrhage, causes enlarged upper airway structures and is likely to cause sudden complete blockage.
Case Presentation
A 7-month-old male infant with a known case of congenital lymphatic malformation in the base of tongue presented in the outpatient department of pediatric surgery. Antenatal history of the infant was uneventful except for this large lymphangioma in the oral cavity. The mother of the infant gave a history of failed remission of the lesion despite repeated bleomycin injections into the lesion under ultrasound guidance at multiple large government centers.
On examination of oral cavity, there was a single globular swelling in the floor of mouth extending bilaterally from mandible to clavicle (Figure 1). The systemic examination revealed no abnormality. Laboratory reports including complete blood count, renal and liver function tests, coagulation profile and chest x-ray were normal. Magnetic Resonance imaging of neck (plain) revealed an irregular T2 heterogenous high intensity lesion in the floor of the mouth along the root of the tongue. Bilateral mandibular space extension was also seen posteriorly, more on the right side with possible involvement of right submandibular gland (Figure 2).

Figure 1: Clinical photograph demonstrating a single globular swelling in the floor of the mouth.
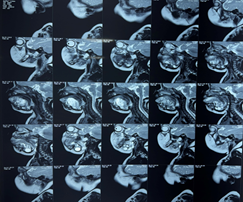
Figure 2: Plain magnetic resonance imaging of the neck revealing an irregular, heterogeneous, T2-hyperintense lesion in the floor of the mouth along the root of the tongue.
Methods (differential diagnosis, investigations and treatment)
The infant was scheduled for surgical excision under general anesthesia, with parents counselled on potential airway challenges, postoperative ventilation, and possible tracheostomy. A multidisciplinary team including anesthesiologists, pediatric and head-neck surgeons, a pediatrician, and PICU nurses---collaborated on management. The plan prioritized oral intubation with tracheostomy backup, ensuring preparedness for airway difficulties. Dedicated anesthesiologists oversaw induction and airway security, while close perioperative monitoring and PICU admission were arranged. The team emphasized meticulous planning to optimize safe surgical and postoperative outcomes.
Despite an 80% oral cavity swelling, bag-mask ventilation was uneventful. Induction included fentanyl (2 mcg/kg), ketamine (2 mg/kg), propofol (40 mg), and sevoflurane (MAC 2) with 100% oxygen. Pre-relaxant laryngoscopy revealed vocal cords after tracheal manipulation, allowing oral intubation with a 3.5mm cuffed flexometallic tube following rocuronium (10 mg). Anesthesia was maintained with sevoflurane (MAC 2), oxygen (2 L/min), and dexamethasone (2 mg). The tongue-base mass was excised meticulously over 2 hours with careful fluid and temperature management (Figure 3). Though reversed with sugammadex (50 mg), extubation was deferred due to tongue edema and airway obstruction risk.
Results
The infant was shifted to PICU. Sedation and mechanical ventilation were maintained overnight. Injection dexamethasone was continued and injection hyaluronidase 250mg was administered locally. The infant was assessed for extubation at 24, 48 and 72 hours postoperatively. However, spontaneous breathing trials were unsuccessful due to persistent tongue edema covering nearly 80% of the oral cavity (Figure 3). Following parental counseling, surgical tracheostomy was performed on the fourth postoperative day (Figure 4). The patient was subsequently shifted back to PICU, gradually weaned, and then transferred to the ward. Decannulation was performed, and the infant was discharged on the thirteenth postoperative day without complications. Follow-up MRI after one month showed no residual disease.
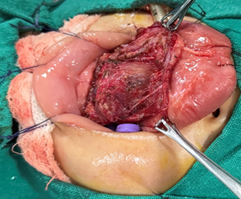
Figure 3: Intraoperative view of the lymphangioma originating from the base of the tongue.

Figure 4: Postoperative photograph showing tongue edema and the surgical tracheostomy site.
Discussion
The treatment of infants with large oral lymphangiomas preoperatively requires heightened attention due to the increased risk of airway compromise, not only during anesthetic induction but also in the immediate postoperative period. In the present case, a 7-month-old infant presented with a giant oral lymphangioma extending to the tongue base.
Direct laryngoscopy was attempted following cautious induction with ketamine, propofol, and sevoflurane, achieving an adequate depth of anesthesia without airway collapse. In pediatric anesthesia, current difficult airway guidelines recommend deferring muscle relaxant administration until the glottis is visualized and ventilation confirmed [8]. Proper placement of a flexometallic endotracheal tube was essential due to its reduced risk of kinking during prolonged head and neck surgery. Maintaining hemodynamic stability and oxygenation during excision required meticulous fluid balance, temperature regulation, and steroid administration to mitigate airway edema.
Persistent tongue edema 72 hours postoperatively necessitated early tracheostomy, consistent with prior recommendations [9]. In this case, tracheostomy provided a definitive airway, facilitating gradual edema resolution while minimizing the risk of acute obstruction.
This case underscores the critical role of a multidisciplinary team in managing complex cases in resource-limited settings, ultimately improving patient outcomes.
Conclusion
Large oral lymphangiomas in infants pose significant anaesthetic risks, necessitating thorough preoperative planning, multidisciplinary coordination, and readiness for emergency airway management. This case highlights the importance of anticipating delayed airway compromise and considering early tracheostomy for extensive lesions to prevent life-threatening obstruction. Further research is needed to refine perioperative strategies for such high-risk patients.
Declarations
Acknowledgments
None.
Author Contributions
Rahul Kumar Chaudhary: conceptualization, writing – original draft, writing – review and editing. Rojina Sedhai: conceptualization.
Satish Kumar Thakur: conceptualization.
Anuja Pokharel: conceptualization.
Kanak Khanal: conceptualization.
Rahul Mahato: conceptualization.
Hiramani Pathak: conceptualization.
Informed consent statement
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement
The authors declare that they have no conflict of interest to disclose.
Care Checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
References
- Grasso DL, Pelizzo G, Zocconi E, Schleef J (2008). Lymphangiomas of the head and neck in children. Acta Otorhinolaryngol Ital.,28:17-20.
Publisher | Google Scholor - Minocha PK, Roop L, Persad R (2014). Cases of Atypical Lymphangiomas in Children. Case Rep Pediatr.,2014:626198.
Publisher | Google Scholor - Kolay SK, Parwani R, Wanjari S, Singhal P (2018). Oral lymphangiomas - clinical and histopathological relations: an immunohistochemically analyzed case series of varied clinical presentations. J Oral Maxillofac Pathol.,22: S108-111.
Publisher | Google Scholor - de Queiroz AM, Silva RA, Margato LC, Nelson-Filho P (2006). Dental care management of a young patient with extensive lymphangioma of the tongue: a case report. Spec Care Dentist.,26:20-24.
Publisher | Google Scholor - Elluru RG, Balakrishnan K, Padua HM (2014). Lymphatic malformations: diagnosis and management. Semin Pediatr Surg.,23:178-185.
Publisher | Google Scholor - Shah AA, Mahmud K, Shah AV (2020). Generalized lymphangioma of the tongue: a rare cause of macroglossia. J Indian Assoc Pediatr Surg.,25:49-51.
Publisher | Google Scholor - Bertino F, Trofimova AV, Gilyard SN, Hawkins CM (2021). Vascular anomalies of the head and neck: diagnosis and treatment. Pediatr Radiol.,51:1162-1184.
Publisher | Google Scholor - Fiadjoe JE, Nishisaki A, Jagannathan N, et al., (2020). Airway management complications in children with difficult tracheal intubation: a report from the Pediatric Difficult Intubation Registry (PeDI-R). Anesthesiology.133(6):1287-1297.
Publisher | Google Scholor - Balakrishnan K, Edwards TC, Perkins JA (2013). Functional and symptom impacts of pediatric head and neck lymphatic malformations: developing a patient-derived instrument. JAMA Otolaryngol Head Neck Surg.,139(10):1090-1096.
Publisher | Google Scholor























