

Case Report
Reconstruction of a Severe Forearm and Wrist Deformity Following Multiple Distal Ulna Tumor Resections: A Case Report
- Ahmad Almigdad *
Department of Orthopedic, Royal Medical Services, Amman, Jordan.
*Corresponding Author: Ahmad Almigdad, Department of Orthopedic, Royal Medical Services, Amman, Jordan.
Citation: Almigdad A. (2026). Reconstruction of a Severe Forearm and Wrist Deformity Following Multiple Distal Ulna Tumor Resections: A Case Report, Clinical Case Reports and Studies, BioRes Scientia Publishers. 12(6):1-7. DOI: 10.59657/2837-2565.brs.26.329
Copyright: © 2026 Ahmad Almigdad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 28, 2026 | Accepted: May 12, 2026 | Published: May 27, 2026
Abstract
Forearm deformities can arise from congenital, traumatic, infectious, neoplastic, or iatrogenic causes, resulting in angular, rotational, or longitudinal misalignment that impairs function and cosmesis. Treatment-related factors, including multiple surgeries, bone loss, and graft failure, as well as chronic degenerative changes can further exacerbate deformity and functional limitation.
We report a case of a 41-year-old female with a history of multiple distal ulna tumor resections since adolescence, resulting in combined angular and rotational deformities of the forearm, limb shortening, and advanced wrist osteoarthritis. The patient underwent corrective osteotomy of the radius, stabilized with dual plating, combined with wrist arthrodesis. Postoperatively, the patient achieved satisfactory alignment, pain relief, and improved overall limb function. This case highlights the long-term consequences of repeated surgical interventions and underscores the importance of comprehensive, biomechanically sound reconstructive planning that addresses both osseous and soft tissue pathology in complex forearm deformities.
Keywords: forearm deformity; distal ulna resection; corrective osteotomy; wrist arthrodesis; reconstructive surgery
Introduction
Forearm deformities can arise from a wide range of congenital, traumatic, infectious, neoplastic, and iatrogenic causes, often resulting in angular, rotational, or longitudinal discrepancies between the radius and ulna [1,2]. These deformities may significantly impair upper limb function and cosmesis, with secondary involvement of the elbow and wrist due to altered forearm biomechanics [3].
Neoplastic and infectious conditions may contribute to forearm deformity either through the primary pathological process or as a consequence of treatment, including tumor resection–related bone loss, radiation-induced growth disturbance, and post-infectious physeal damage. Iatrogenic factors represent an important and potentially preventable cause of forearm deformity and include multiple surgical resections, excessive bone removal, failed reconstruction, implant failure, bone graft resorption, and the formation of radioulnar bony bridges or synostosis. Degenerative and functional sequelae—such as chronic distal radioulnar joint instability, untreated distal ulna resection, and long-standing wrist arthritis with carpal malalignment—may further exacerbate deformity and functional limitation [4–6].
In this report, we present the case of a 41-year-old female with a severe forearm and wrist deformity following multiple distal ulna tumor resections, resulting in combined angular and rotational forearm deformities and advanced wrist osteoarthritis. The patient was treated with corrective radial osteotomy combined with wrist arthrodesis. This case highlights the long-term consequences of repeated surgical interventions and underscores the importance of comprehensive reconstructive planning to restore alignment, relieve pain, and minimize functional impairment.
Case Presentation
A 41-year-old female with no known medical comorbidities presented to the upper limb clinic with complaints of left forearm deformity and severe wrist pain. The patient reported a history of approximately 14 surgical procedures performed over several years for a presumed benign tumor of the distal ulna. However, she was unable to provide medical records and could not recall detailed information regarding the exact diagnosis or specific surgical interventions, as all treatments had been carried out at institutions outside our center more than 20 years earlier.
Her symptoms began at the age of 14, when she noticed diffuse swelling of the left forearm. Initial investigations reportedly revealed a benign tumor involving the distal ulna. Over the subsequent years, she underwent multiple surgical procedures, including tumor resection and two bone grafting procedures harvested from both fibulae, performed approximately one year apart. Additional surgeries were reportedly undertaken to address implant failure and graft resorption. The patient denied any history of postoperative infection and did not recall receiving adjuvant therapies such as radiotherapy. At approximately 20 years of age, she was advised by her treating physician that further surgical intervention carried a significant risk of limb loss, including possible amputation. Consequently, she refrained from seeking further medical care despite persistent symptoms.
More than two decades later, the patient presented with worsening symptoms, including severe wrist pain, a visible bowing deformity of the forearm, and limb shortening. The pain was activity-related and associated with cold intolerance. She reported significant functional limitations, including restricted wrist and forearm motion and inability to actively extend the thumb.
On physical examination, there was pronounced dorsal angulation of the forearm at the mid-shaft level, accompanied by marked deformity and shortening (Figure 1). The wrist was internally rotated approximately 90 degrees relative to the elbow. A wide, unsightly scar measuring approximately 10 cm extended along the radial aspect of the forearm and wrist. A skin cleft was noted over the dorsal wrist, with underlying bone palpable beneath the scar. The extensor pollicis longus tendon was not palpable, and active thumb extension was absent. Sensory examination revealed decreased sensation over the radial aspect of the forearm and the first web space, consistent with superficial radial nerve involvement. Elbow flexion and extension were comparable to the contralateral side; however, forearm supination was severely restricted, limited to approximately 10 degrees short of the mid-prone position. Wrist motion was markedly restricted and painful in all planes, while sensation elsewhere in the limb was intact.

Figure 1: Preoperative clinical photographs of the left forearm. (A) Dorsal view of both forearms demonstrating shortening and deformity of the left forearm. (B) Limited supination of the left forearm. (C) Radial view showing a long, wide scar extending along the radial aspect of the forearm and the dorsoradial aspect of the wrist, associated with forearm deformity and volar subluxation of the wrist. (D) Dorsal view of the left upper limb demonstrating forearm deformity with swelling and angular malalignment.
Radiological evaluation revealed a severe post-surgical deformity of the forearm following multiple tumor resections, characterized by limb shortening and marked malalignment of the radius and ulna (Figure 2). The distal ulna had been resected, with formation of a bony bridge extending from the ulna to the wrist. The wrist demonstrated significant carpal malalignment and advanced degenerative changes, including volar subluxation. Computed tomography provided a detailed assessment of the complex deformity and rotational malalignment of the radius (Figure 3). CT angiography was performed to exclude vascular compromise given the extent of deformity and prior surgeries.

Figure 2: Preoperative plain radiographs of the forearm and wrist demonstrating severe post-surgical deformity following multiple tumor resections. (A) Anteroposterior and (B) lateral views of the forearm showing marked angular deformity, shortening, and altered alignment of the radius and ulna, with resection of the distal ulna and a bony bridge extending between the ulna and the wrist. (C) Anteroposterior and (D) lateral views of the wrist demonstrating significant carpal malalignment and advanced degenerative changes.
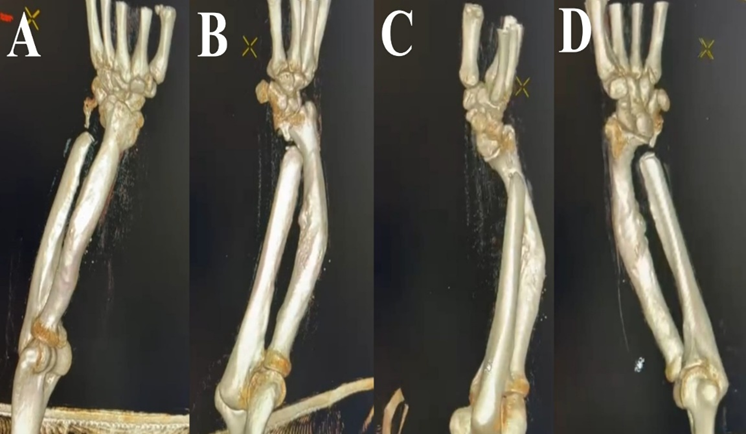
Figure 3: Three-dimensional CT reconstructions (A–D) from different angles demonstrating angular and rotational deformity of the radius, associated with distal ulna resection and a bony bar extending from the ulna toward the wrist.
Surgical Technique
The decision to proceed with wrist arthrodesis and corrective radial osteotomy was discussed with the patient, who agreed to and expressed satisfaction with the proposed treatment plan. Surgery was performed under general anesthesia with an additional regional block, using tourniquet control. A dorsal approach to the wrist was utilized, and the skin incision was extended over the radial shaft, planned along the border of the existing scar to allow excision of excessive scar tissue while preserving normal skin (Figure 4). The radial shaft was exposed at the apex of the deformity, and surrounding soft tissues were carefully stripped from the bone.
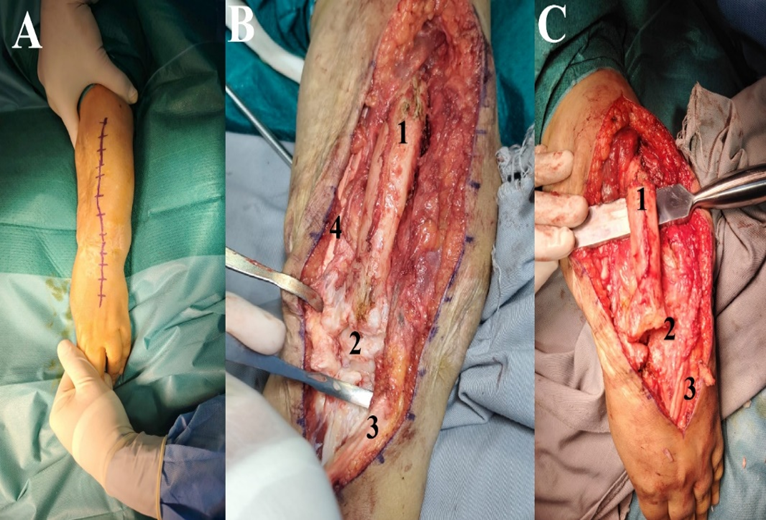
Figure 4: Intraoperative images. (A) Preoperative skin markings demonstrating the planned dorsal wrist approach and an incision along the ulnar border of the existing scar. (B, C) Intraoperative exposure of the radial shaft showing marked widening and angular deformity of the radius. (1: Radius; 2: Wrist joint—shown in B prior to capsulotomy and in C after capsulotomy; 3: Contents of the fourth dorsal compartment, including the extensor digitorum communis tendons; 4: Extensor carpi radialis brevis tendon).
The extensor retinaculum was opened over the fourth dorsal compartment. The third compartment, which normally contains the extensor pollicis longus tendon, was absent. The second dorsal compartment, containing the extensor carpi radialis longus and brevis tendons, was displaced radially due to the forearm bowing deformity. A dorsal capsulotomy was performed, followed by proximal row carpectomy and preparation of the wrist arthrodesis site.
A closing wedge osteotomy was performed dorsally at the center of rotation of angulation (CORA) of the radial shaft, with concomitant shortening of the radius to reduce tension on the soft tissues after correction of the deformity. The osteotomy was stabilized using dual plating: a 7-hole locking compression plate applied laterally with three screws proximally and three distally, and an additional 7-hole reconstruction plate applied dorsally with two screws proximally and two distally. Dual plating was chosen to enhance rotational stability and load sharing, given the abnormal bone geometry and compromised bone quality. Wrist arthrodesis was then performed and fixed using a 30-degree fusion plate (Figure 5). Correction of the rotational deformity was achieved at the wrist level, resulting in the radial styloid assuming a volar orientation. Autologous bone graft harvested from the carpectomy specimen, combined with demineralized bone matrix, was applied to both the fusion and osteotomy sites.
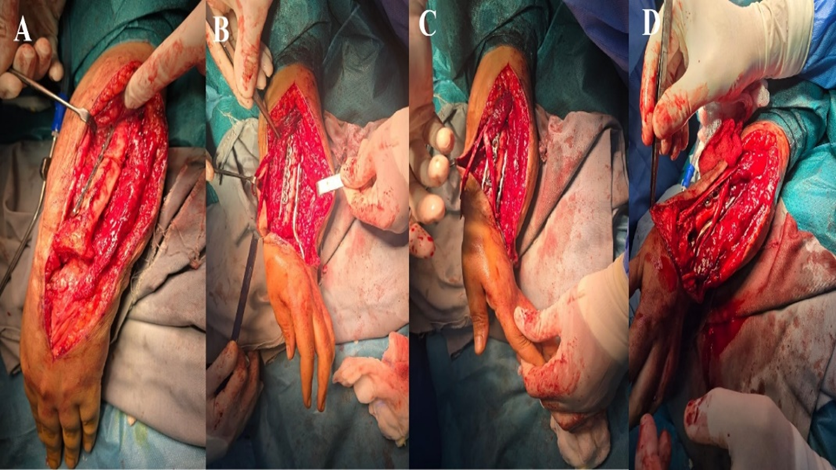
Figure 5: Intraoperative images following corrective osteotomy and wrist arthrodesis. (A) Closing wedge osteotomy performed at the center of rotation of angulation (CORA) of the radial shaft, stabilized with a 7-hole plate applied to the radial aspect of the radius. (B) Correction of the rotational deformity at the wrist level, achieved by volar rotation of the carpal bones, resulting in the radial styloid assuming a volar orientation. Wrist arthrodesis was performed using a 30-degree angled fusion plate, with an additional 7-hole reconstruction plate applied to the lateral aspect of the radius. (C) Corrected wrist position following osteotomy and arthrodesis, with exposure of the extensor carpi radialis longus and brevis tendons. (D) Tendon transfer using the extensor carpi radialis longus to reconstruct the extensor pollicis longus.
The extensor pollicis brevis tendon was explored, and a distal stump was identified at the wrist level. Tendon transfer was performed by transferring the extensor carpi radialis longus to the extensor pollicis longus, and the extensor carpi radialis brevis tendon was resected. The tourniquet was then deflated, meticulous hemostasis was achieved, and the wound was closed in layers. An above-elbow cast was applied postoperatively. Postoperatively, forearm malrotation was corrected, with the wrist aligned in the same plane as the elbow joint (Figure 6), and the corresponding X-ray is shown in Figure 7.
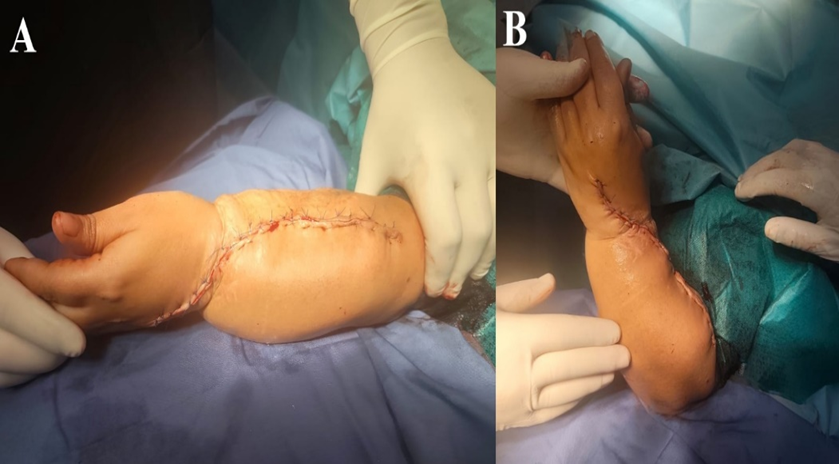
Figure 6: Postoperative clinical photographs. (A, B) Images demonstrating relocation of the forearm scar to the radial aspect of the forearm following deformity correction, with restoration of forearm rotational and angular alignment, improvement of wrist pronation, and alignment of the wrist in the same plane as the elbow.
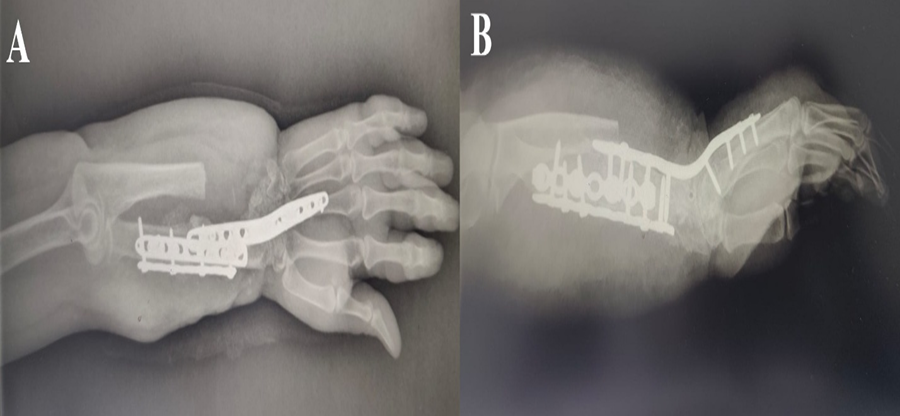
Figure 7: Postoperative plain radiographs of the forearm and wrist. (A) Anteroposterior and (B) lateral views demonstrate corrective osteotomy at the level of the radius stabilized with dual plate fixation, along with wrist arthrodesis fixed in approximately 30 degrees of extension.
Discussion
The forearm functions as an integrated anatomical and biomechanical unit, with coordinated interaction between the radius and ulna enabling pronation–supination while transmitting load from the hand to the elbow [7]. Disruption of this relationship—particularly following distal ulna resection without adequate reconstruction—can markedly disturb normal forearm biomechanics [8]. Prior reports have demonstrated that inadequately treated distal ulna defects may result in radial bowing, proximal migration of the radius, increased radiocarpal loading, carpal malalignment, and progressive degenerative changes of the wrist [9]. In the present case, the combined effects of multiple surgical resections, failed bone grafting, and probable growth disturbance during adolescence led to progressive deformity, forearm shortening, and subsequent functional deterioration of the wrist.
Iatrogenic factors can play a significant role in the development of bony deformity, particularly when surgical interventions are performed during periods of skeletal growth [10]. Repeated operations may result in excessive bone loss, disrupted growth patterns, extensive scarring, tendon attrition, and the formation of radioulnar synostosis or bony bridging [2]. These long-term sequelae highlight the importance of careful surgical planning in managing forearm pathologies, especially in young patients, with an emphasis on preserving forearm length, alignment, and joint integrity whenever possible.
Treatment of complex, multiplanar forearm deformities requires meticulous preoperative evaluation and a thorough understanding of the underlying pathology. In the present case, performing the corrective osteotomy at the center of rotation of angulation (CORA) enabled accurate restoration of forearm alignment while minimizing secondary translation and soft tissue strain. Dual-plate fixation provided stable and reliable stabilization despite abnormal bone morphology and compromised bone quality.
The decision to proceed with wrist arthrodesis was guided by advanced degenerative changes, carpal malalignment, and severe pain with minimal residual motion, as motion-preserving reconstructive options were unlikely to provide durable pain relief or functional improvement. Wrist arthrodesis remains a reliable solution for pain control and stability in end-stage wrist arthritis, particularly when combined with correction of forearm alignment. In our patient, arthrodesis also helped correct residual rotational deformity at the wrist, contributing to improved overall limb alignment.
Although transfer of the extensor carpi radialis longus (ECRL) to the extensor pollicis longus (EPL) is not commonly performed, it was selected in this case because wrist arthrodesis renders the ECRL functionally redundant, allowing its use without donor-site morbidity. Successful outcomes in such complex reconstructions depend on addressing both osseous and soft tissue pathology, rather than focusing solely on bony correction.
This case highlights the challenges of managing severe forearm and wrist deformities resulting from multiple prior interventions. Comprehensive preoperative planning, careful restoration of bony alignment, and strategic soft tissue management are essential to achieve functional improvement and pain relief. Combined bony and soft tissue procedures can provide a reliable solution in complex cases and help optimize long-term outcomes.
Conclusion
Forearm deformities can arise from congenital, traumatic, infectious, neoplastic, or iatrogenic causes, either directly or as a consequence of treatment, such as bone loss from tumor resection, radiation-induced growth disturbances, or post-infectious physeal damage. Iatrogenic factors-including multiple surgeries, excessive bone resection, failed reconstruction, implant failure, and bone graft resorption-can further contribute to deformity. Additionally, chronic degenerative changes may exacerbate malalignment and functional impairment.
References
- Chan, C. X., Song, J., Woo, C. Y., Lam, K. Y., Puhaindran, M. E., Ning, B., & Hui, H. P. J. (2025). A new classification system for forearm deformities caused by hereditary multiple osteochondromas. Journal of Hand Surgery (American Volume), 50(8):1006.e1–1006.e10.
Publisher | Google Scholor - Massobrio, M., Pellicanò, G., Albanese, P., & Antonietti, G. (2014). Forearm post-traumatic deformities: Classification and treatment. Injury, 45(2):424–427.
Publisher | Google Scholor - Jupiter, J. B., & Fernandez, D. L. (2001). Complications following distal radial fractures. Journal of Bone and Joint Surgery (American Volume), 83(8):1244–1265.
Publisher | Google Scholor - Collado-Torres, F., Zamora-Navas, P., & de la Torre-Solís, F. (1995). Secondary forearm deformity due to injury to the distal ulnar physis. Acta Orthopaedica Belgica, 61(3):242–244.
Publisher | Google Scholor - Müller-Färber, J. A., & Schläger, B. (2008). Secondary forearm deformity due to premature closure of the distal ulnar physis. Unfallchirurg, 111(2):117–121.
Publisher | Google Scholor - Kolovich, G. P., Heifner, J. J., Falgiano, P. A., & Mahoney, B. (2024). Distal radioulnar joint instability. Journal of Orthopaedic Trauma, 38(Suppl. 9):S4–S10.
Publisher | Google Scholor - Mader, K., Koolen, M., Flipsen, M., et al. (2015). Complex forearm deformities: Operative strategy in posttraumatic pathology. Obere Extremität, 10:229–239.
Publisher | Google Scholor - Barbaric, K., Rujevcan, G., Labas, M., Delimar, D., & Bicanic, G. (2015). Ulnar shortening osteotomy after distal radius fracture malunion: Review of the literature. Open Orthopaedics Journal, 9:98–106.
Publisher | Google Scholor - Barinaga, G., Rodriguez-Feo, C., Rasmussen, E., Telfer, S., & Iannuzzi, N. (2022). The effect of forearm shortening on forearm range of motion. Journal of Hand Surgery (American Volume), 47(1):87.e1–87.e7.
Publisher | Google Scholor - Peterson, H. A. (2006). Physeal injuries and growth disturbances. In R. T. Morrissy & S. L. Weinstein (Eds.), Lovell and Winter’s pediatric orthopaedics. Lippincott Williams & Wilkins, 6th ed.,:125–167.
Publisher | Google Scholor























