

Research Article
Molecular Determinants of Antibiotic Resistance in Klebsiella Pneumoniae Isolates from Septicaemia Cases in ICU Patients
1 Microbiology, Adviser Specialist in Pathology, Deputy Commandant, AFIP, Dhaka Cantonment, Bangladesh.
2 Microbiology, AFIP, Dhaka Cantonment, Bangladesh.
*Corresponding Author: Monirul Hoque, Microbiology, Adviser Specialist in Pathology, Deputy Commandant, AFIP, Dhaka Cantonment, Bangladesh.
Citation: Hoque M, Haque S, Kausar H. (2026). Molecular Determinants of Antibiotic Resistance in Klebsiella Pneumoniae Isolates from Septicaemia Cases in ICU Patients, Journal of BioMed Research and Reports, BioRes Scientia Publishers. 10(5):1-07. DOI: 10.59657/2837-4681.brs.26.248
Copyright: © 2026 Monirul Hoque, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 16, 2026 | Accepted: April 13, 2026 | Published: April 27, 2026
Abstract
Background: Klebsiella pneumoniae is a prominent pathogen linked to septicemia, especially among patients in intensive care units (ICUs), where it poses a significant risk due to its growing antimicrobial resistance. In Bangladesh, there is a lack of updated, localized data regarding its resistance trends, particularly in critical care environments.
Materials and Methods: This cross-sectional study was conducted over 03 years (July 2021 - June 2024) in the ICUs of two tertiary hospitals in Dhaka. Blood samples from 301 patients with suspected septicemia were analyzed using automated culture and identification systems. Antimicrobial susceptibility testing was performed using the disc diffusion method, following the Clinical and Laboratory Standards Institute (CLSI) guidelines. Additionally, 11 multidrug-resistant K. pneumoniae isolates were subjected to PCR (Polymerase Chain Reaction) to detect specific resistance genes.
Results: Out of the 301 septicemic cases, 64.8% were male. Gram-negative bacteria dominated the isolates, with K. pneumoniae being the second most common organism (25.2%). These isolates showed high resistance to multiple antibiotics, including ceftazidime (84.2%), cotrimoxazole (80.3%), and ceftriaxone (75.0%). Notably, 48.7% of isolates were resistant to meropenem. However, colistin (5.3%) and tigecycline (1.3%) remained relatively effective. Molecular analysis revealed that all selected K. pneumoniae strains carried key resistance genes such as blaCTX-M, blaNDM-1, blaOXA-48, blaSHV, blaTEM, and mphA. The blaCTX-M-15 gene was also highly prevalent (90.91%), where as blaKPC and blaCTX-M-9 were not detected.
Conclusion: The high rate of resistance in K. pneumoniae isolates from ICU patients, along with the presence of multiple resistance genes, underscores a critical need for strengthened infection control practices, routine molecular surveillance, and judicious antibiotic use in ICUs settings. Addressing this growing threat is essential to improve patient outcomes and contain antimicrobial resistance in Bangladeshi healthcare facilities.
Keywords: intensive care unit (ICU), clinical and laboratory standards institute (CLSI), blaCTX-M-15, blaNDM-1, blaOXA-48, blaSHV, blaTEM, mphA, blaKPC, PCR (polymerase chain reaction)
Introduction
Septicemia, a life-threatening bloodstream infection, is a significant cause of morbidity and mortality in intensive care units (ICUs) worldwide. Critically ill patients are particularly vulnerable due to their compromised immunity, frequent exposure to invasive procedures, prolonged hospital stays, and the routine use of broad-spectrum antibiotics (Vincent et al., 2009). Among the diverse pathogens implicated in septicemia, Klebsiella pneumoniae has emerged as a major concern, especially in ICU settings, due to its dual capability of causing severe infections and developing multidrug resistance (Podschun & Ullmann, 1998; Pitout et al., 2008).
Klebsiella pneumoniae, a Gram-negative bacterium belonging to the Enterobacteriaceae family, is responsible for a broad spectrum of healthcare-associated infections (HAIs), including pneumonia, urinary tract infections, wound infections, and most critically, bloodstream infections. In ICUs, its prevalence is heightened by environmental persistence and its ability to colonize indwelling medical devices such as catheters and ventilators (Nordmann et al., 2011). The rise in antibiotic-resistant K. pneumoniae strains has posed a significant therapeutic challenge, often leaving clinicians with limited treatment options and increased patient management complexity.
The pathogen’s adaptability is largely due to its acquisition of multiple resistance genes, often carried on plasmids and other mobile genetic elements, enabling rapid dissemination among bacterial populations (Logan & Weinstein, 2017). Particularly alarming is the global spread of extended-spectrum β-lactamases (ESBLs), which confer resistance to third-generation cephalosporins, and carbapenemases such as NDM-1, KPC, and OXA-48, which degrade carbapenems-considered last-line agents for many Gram-negative infections (Nordmann et al., 2011; Cantón et al., 2012). These mechanisms have led to the emergence of multidrug-resistant (MDR), extensively drug-resistant (XDR), and in some cases, pan-drug-resistant (PDR) K. pneumoniae strains.
The World Health Organization (WHO) has identified carbapenem-resistant K. pneumoniae as a “critical priority” pathogen, underscoring the urgent need for new antibiotics and effective infection control strategies (WHO, 2017). The situation is especially dire in low- and middle-income countries (LMICs), where the unregulated use of antibiotics, lack of standardized treatment protocols, and insufficient diagnostic infrastructure contribute to the rapid evolution and spread of resistant strains (Laxminarayan et al., 2013; Gandra et al., 2016).
Despite the growing global attention to antimicrobial resistance (AMR), there is a paucity of local data from ICU environments in Bangladesh that comprehensively capture both the phenotypic and molecular profiles of resistant K. pneumoniae. Most healthcare institutions lack routine molecular diagnostic tools, making it difficult to identify key resistance genes such as blaNDM-1, blaOXA-48, blaCTX-M, and others that critically influence treatment decisions.
This study was designed to address this gap by investigating the antibiotic resistance patterns of Klebsiella pneumoniae isolated from blood cultures of septicemic ICU patients in two tertiary care hospitals in Dhaka. In addition to standard antimicrobial susceptibility testing, a subset of multidrug-resistant isolates was subjected to molecular characterization to identify specific resistance genes using polymerase chain reaction (PCR). By correlating phenotypic resistance with genetic determinants, this study aims to enhance our understanding of resistance mechanisms and inform the development of more targeted antimicrobial therapy and infection control strategies in ICU settings.
Materials and Methods
Study Setting
This observational cross-sectional study was under taken in the Intensive Care Units, Combined Military Hospital (CMH), Dhaka and Kurmitola General Hospital (KGH), Dhaka Cantonment; two tertiary level hospitals in Dhaka, Bangladesh from July 2021 to June 2024. A total 301 hospitalized cases of clinically suspected septicemia were enrolled. A thorough physical examination was carried out after taking detailed and careful history of each case. Patient’s attendants were interviewed and only those were enrolled where the legal guardians gave permission for collection of samples.
Ethical Approval
Ethical clearance was taken from Ethical Review Committee of the Directorate General of Medical Services (DGMS) and the authority of Kurmitola General Hospital (KGH), Dhaka. Informed consent was obtained from the patients or from patient’s legal guardians by protecting anonymity.
Confirmation of K. Pneumoniae Isolates
As a sample, 8-10 ml of blood was withdrawn aseptically into specific blood culture bottles. Inoculated culture bottles were incubated at 37°C aerobically in Automated Blood Culture System BD BACTEC FX. For positive signals the samples were inoculated on blood agar and MacConkey’s agar media followed by incubation at 37°C aerobically. The growth, if obtained was identified by colony morphology, Gram’s stain and conventional biochemical tests. For maintaining the highest level of accuracy isolated pure colonies of all bacterial isolates were also confirmed by Automated Microbial Identification system (BD Phoenix M50). Bacterial identification was also confirmed by MALDI-TOF (matrix-assisted laser desorption/ ionization time-of-flight) mass spectrometry technology (BIOMÉRIEUX, USA)
Determination of Antibiotic Susceptibility Pattern
The antibiotic susceptibility test of the isolated organism was performed by Kirby-Bauer disc diffusion method on Mueller-Hinton agar media as per the Clinical and Laboratory Standards Institute (CLSI) guidelines (32nd edition) and their sensitivity pattern was noted down. If clinicians ask for MIC of individual bacteria, sample was run in BD Phoenix M50, (USA origin).
Molecular Detection
Eleven of the isolated Multidrug resistant K. pneumonia were selected for molecular characterization by PCR method. PCR amplification of genes was performed with GoTaq Green Master Mix (Promega, USA) by C1000 Touch PCR thermal cycler, (BioRad, USA). All PCR amplicons were verified by gel electrophoresis on a 1.5% agarose gel electrophoresis (Biometra-Agaorese gel mini, Germany), stained with Ethidium bromide (1 μl/ml) for 30 min under 100V in 1X TAE buffer and visualized by GelDoc Go Imaging System (BioRad, USA). PCR amplicon sizes were calculated by a comparison with 100 bp molecular weight DNA ladder (BioLabs, USA). PCR Primers Used in the Study are:
| Gene | Primer Used | Amplicon Size (bp) | References |
| blaTEM | F: CATTTCCGTGTCGCCCTTAT | 793 | (Randall et al., 2004) |
| R: TCCATAGTTGCCTGACTCCC | |||
| blaCTX-M | F: ATGTGCAGYACCAGTAARGTKATGGC | 592 | (Gundran et al., 2019) |
| R: TGGGTRAARTARGTSACCAGAAYSAGCGG | |||
| blaCMY | F: TGGCCAGAACTGACAGGCAAA | 462 | (Mandakini et al., 2020) |
| R: TTTCTCCTGAACGTGGCTGGC | |||
| blaSHV | F: TCGCCTGTGTATTATCTCCC | 768 | (Van et al., 2008) |
| R: CGCAGATAAATCACCACAATG | |||
| blaKPC | F: CGTCTAGTTCTGCTGTCTTG | 798 | (Poirel et al., 2011) |
| R: CTTGTCATCCTTGTTAGGCG | |||
| blaCTX-M-15 | F: CACACGTGGAATTTAGGGACT | 996 | (Paterson et al., 2003) |
| R: GCCGTCTAAGGCGATAAACA | |||
| blaCTX-M-2 | F: CGGTGCTTAAACAGAGCGAG | 624 | (Thabit et al., 2011) |
| R: CCATGAATAAGCAGCTGATTGCCC | |||
| blaCTX-M-8 | F: ACGCTCAACACCGCGATC | 490 | (Thabit et al., 2011) |
| R: CGTGGGTTCTCGGGGATAA | |||
| blaCTX-M-9 | F: GATTGACCGTATTGGGAGTTT | 947 | (Thabit et al., 2011) |
| R: CGGCTGGGTAAAATAGGTCA | |||
| blaNDM1 | F: GGTTTGGCGATCTGGTTTTC | 621 | (Poirel et al., 2011) |
| R: CGGAATGGCTCATCACGATC | |||
| blaOXA-48 | F: GCGTGGTTAAGGATGAACAC | 438 | (Poirel et al., 2011) |
| R: CATCAAGTTCAACCCAACCG | |||
| blaCMY-2 | F: TGGCCGTTGCCGTTATCTAC | 870 | (Torkan, Khamesipour and Anyanwu, 2015) |
| R: CCCGTTTTATGCACCCATGA | |||
| mphA | F: GTGAGGAGGAGCTTCGCGAG | 403 | (Nguyen et al., 2009) |
| R: TGCCGCAGGACTCGGAGGTC |
Results
We analyze 301 septicaemic patients in the ICU by sex. Among the patients, 64.8% (195 individuals) were male, while 35.2% (106 individuals) were female (Figure 1). This indicates a higher prevalence of septicemia among male patients in the study population.
Figure 1: Distribution of septicemic patients admitted in ICUs according to their sex (n=301).
The distribution of bacterial isolates responsible for septicemia was detailed in Table 1. Gram-negative organisms predominated, with Burkholderia cepacia complex leading at 26.9%, followed closely by Klebsiella spp at 25.2% and Escherichia coli at 24.9%. Acinetobacter spp accounted for 15.3% of cases, while Pseudomonas spp and Serratia marcescens were less common, contributing 7.0% and 0.3%, respectively. Gram-positive organisms were notably sparse, with Staphylococcus aureus comprising just 0.3% of cases. These findings underscore the diversity and prevalence of bacterial pathogens causing septicemia in critically ill patients, highlighting the importance of targeted infection control measures and effective treatment strategies in intensive care settings.
Table 1: Frequency of bacterial isolates responsible for septicemia among ICU admitted patients (n=301).
| Organism | Frequency (n) | Percentage (%) |
| Gram Negative Organisms | ||
| Burkholderia cepacia complex | 81 | 26.9 |
| Klebsiella spp | 76 | 25.2 |
| Escherichia coli | 75 | 24.9 |
| Acinetobacter spp | 46 | 15.3 |
| Pseudomonas spp | 21 | 7 |
| Serratia marcescens | 1 | 0.3 |
| Gram Positive Organisms | ||
| Staphylococcus aureus | 1 | 0.3 |
Percentage of bacterial isolates responsible for septicemia among ICU admitted patients is Klebsiella spp (25.2%) and others 74.8% (Burkholderia cepacia complex, Escherichia coli, Acinetobacter spp, Pseudomonas spp and Serratia marcescens).
Figure 2: Percentage of bacterial isolates responsible for septicemia among ICU admitted patients (n=301).
Resistant pattern of Klebsiella spp. Isolated from blood cultures in a study involving 76 cases, several concerning trends in antibiotic resistance are evident. The highest resistance rates were observed against cotrimoxazole (80.3%), ceftazidime (84.2%), and cefixime (80.3%). Resistance was also notably high for ciprofloxacin (67.1%), ceftriaxone (75.0%), and amoxicillin+clavulanic acid (76.3%). Meropenem and colistin showed lower resistance rates at 48.7% and 5.3%, respectively, while tigecycline exhibited the lowest resistance rate at 1.3%.
Table 2: Resistance pattern of Klebsiella spp. Isolated from blood culture in the study (n=76).
| Antibiotic | Resistance Pattern | |
| Frequency (n) | Percentage (%) | |
| Cotrimoxazole | 61 | 80.3 |
| Ciprofloxacin | 51 | 67.1 |
| Ceftriaxone | 57 | 75.0 |
| Gentamicin | 45 | 59.2 |
| Amoxicillin + Clavulanic acid | 58 | 76.3 |
| Ceftazidime | 64 | 84.2 |
| Amikacin | 41 | 53.9 |
| Aztreonam | 57 | 75.0 |
| Meropenem | 37 | 48.7 |
| Netilmicin | 46 | 60.5 |
| Cefixime | 61 | 80.3 |
| Cefepime | 55 | 72.4 |
| Tazobactam+ Piperacillin | 38 | 50.0 |
| Colistin | 4 | 5.3 |
| Tigecycline | 1 | 1.3 |
Distribution of different antibiotic resistance genes in randomly selected Klebsiella pneumoniae isolates (n=11). The blaCMY gene was found in 9.09% of the isolates, while the blaCMY-2 and blaCTX-M-8 genes were present in 81.82% of the isolates. Notably, blaCTX-M, blaCTX-M-2, blaNDM1, blaOXA-48, blaSHV, blaTEM 793, and mphA genes were detected in 100% of the isolates. The blaCTX-M-15 gene was present in 90.91% of the isolates, whereas the blaCTX-M-9 and blaKPC genes were not detected in any of the isolates.
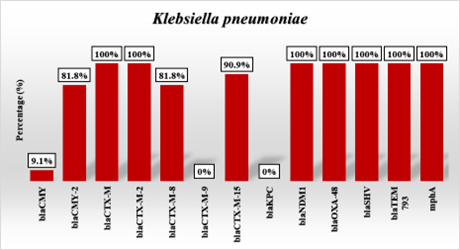
Figure 3: Distribution of different antibiotic resistance genes for randomly selected Klebsiella pneumoniae (n=11).
Discussion
Septicemia remains a major global health concern, particularly among critically ill patients in intensive care units (ICUs), where the risk of acquiring severe infections is amplified due to invasive procedures, prolonged hospitalization, immunosuppression, and antibiotic pressure. In our study of 301 ICU patients with bloodstream infections, we observed a pronounced male predominance (64.8%), reflecting findings from previous studies that report higher infection rates in males across various clinical contexts (Karlsson et al., 2019; Sligl et al., 2015). While the exact reasons remain complex and multifactorial, hypotheses include sex-based immunological differences, behavioral risk factors, and healthcare exposure.
The microbial profile of septicemia in our cohort was dominated by Gram-negative organisms, with Burkholderia cepacia complex, Klebsiella spp., and Escherichia coli as the leading causative agents. The prevalence of Klebsiella spp. (25.2%) aligns with the global recognition of Klebsiella pneumoniae as one of the foremost causes of healthcare-associated infections, including pneumonia, urinary tract infections, and bloodstream infections, particularly in ICU settings (Munoz-Price et al., 2013; Pitout et al., 2015). The low incidence of Gram-positive organisms, such as Staphylococcus aureus (0.3%), is noteworthy and might reflect localized antimicrobial use patterns or effective infection control measures targeting common Gram-positive pathogens.
The antimicrobial susceptibility patterns in our Klebsiella isolates reveal a worrisome level of multidrug resistance. Alarmingly, over 80% of isolates demonstrated resistance to commonly used antibiotics, such as ceftazidime, cefixime, and cotrimoxazole. Resistance rates were also high for ciprofloxacin (67.1%) and amoxicillin-clavulanate (76.3%), echoing the declining efficacy of these drugs in treating Enterobacteriaceae infections across South and Southeast Asia (Gandra et al., 2016; Jean et al., 2022). Third-generation cephalosporins and fluoroquinolones, once considered mainstays in the treatment of Gram-negative bacteremia, now offer limited utility in many clinical settings due to escalating resistance rates.
More concerning is the finding that 48.7% of isolates were resistant to meropenem, a carbapenem considered the drug of last resort for extended-spectrum β-lactamase (ESBL)-producing organisms. This highlights the growing prevalence of carbapenemase-producing K. pneumoniae (CPKP), which is associated with high mortality and limited therapeutic options (van Duin & Doi, 2017). While resistance to colistin (5.3%) and tigecycline (1.3%) remained relatively low, these agents are far from ideal due to their toxicity profiles and pharmacokinetic limitations, and resistance is already emerging in other global hotspots (Olaitan et al., 2014).
Molecular analysis of selected K. pneumoniae isolates provides critical insights into the genetic mechanisms underpinning the observed resistance. All isolates (100%) harbored blaCTX-M, blaTEM, blaSHV, and blaNDM-1 genes. These genes are among the most widespread β-lactamase and carbapenemase determinants globally, with blaCTX-M-15 and blaNDM-1 particularly implicated in numerous hospital outbreaks and endemic spread in Asia and the Middle East (Cantón et al., 2012; Nordmann et al., 2011).
The blaCTX-M family encodes for ESBLs capable of hydrolyzing third-generation cephalosporins, and the predominance of the CTX-M-15 variant (90.91% in our study) is of great clinical relevance. It has been reported across continents and is associated with increased virulence and community spread (Bevan et al., 2017). The co-occurrence of multiple ESBL genes (TEM, SHV, and CTX-M) within the same isolates suggests synergistic mechanisms contributing to high-level resistance.
The presence of blaNDM-1 and blaOXA-48 carbapenemase genes in all isolates is a major cause for concern. NDM-1, first reported in 2008, has rapidly spread across healthcare systems worldwide and is notoriously difficult to treat due to its broad substrate profile and plasmid-mediated transferability (Kumarasamy et al., 2010). Similarly, OXA-48 produces low-level carbapenem resistance that can evade detection by routine susceptibility testing, further complicating infection control efforts.
Additionally, the detection of blaCMY-2 (81.82%)-an AmpC β-lactamase-indicates evolving resistance even beyond traditional ESBLs, contributing to cephalosporin and β-lactam/β-lactamase inhibitor resistance. The detection of the macrolide resistance gene mphA, although not directly implicated in β-lactam resistance, is indicative of a multidrug resistance gene pool that could facilitate horizontal gene transfer and future co-resistance patterns (Zankari et al., 2012).
These findings have grave implications for ICU management and antimicrobial stewardship. The high prevalence of multidrug-resistant and carbapenem-resistant K. pneumoniae underscores the urgent need for robust infection control protocols, including surveillance cultures, contact precautions, and environmental decontamination. The data also support the need for routine molecular diagnostics to identify resistance genes, particularly in high-risk patients or outbreak scenarios.
At the national and global levels, these results call for stronger antimicrobial resistance (AMR) surveillance programs, stewardship initiatives to curb inappropriate antibiotic use, and investment in the development of novel antimicrobial agents or alternative therapies such as bacteriophage therapy and immunomodulation.
Conclusion
This study reveals a high burden of multidrug-resistant Gram-negative bacteria, particularly Klebsiella pneumoniae, among ICU patients with septicaemia in Dhaka. The isolates demonstrated extensive resistance to commonly used antibiotics, including third-generation cephalosporins, fluoroquinolones, and even carbapenems. Molecular characterization further confirmed the widespread presence of carbapenemase and ESBL genes, such as blaNDM-1, blaOXA-48, and blaCTX-M variants, underscoring the severity of antimicrobial resistance in the ICU setting.
The emergence of such highly resistant pathogens represents a significant public health threat, potentially leading to treatment failure, increased morbidity and mortality, and healthcare costs. Immediate and coordinated interventions, including routine surveillance, rational antibiotic use, and molecular diagnostics, are essential to combat this growing crisis in Bangladesh and similar healthcare environments.
References
- Bevan, E.R., Jones, A.M., Hawkey, P.M. (2017). Global epidemiology of CTX-M β-lactamases: Temporal and geographical shifts in genotype. Journal of Antimicrobial Chemotherapy, 72(8):2145-2155.
Publisher | Google Scholor - Cantón, R., González-Alba, J.M., Galán, J.C. (2012). CTX-M enzymes: origin and diffusion. Frontiers in Microbiology, 3:110.
Publisher | Google Scholor - Gandra, S., Barter, D.M., Laxminarayan, R. (2016). Economic burden of antibiotic resistance: how much do we really know. Clinical Microbiology and Infection, 20(10):973-980.
Publisher | Google Scholor - Gandra, S., Mojica, N., Klein, E.Y., Ashok, A., Nerurkar, V., et al. (2016). Trends in antibiotic resistance among major bacterial pathogens isolated from blood cultures tested at a large private laboratory network in India, 2008-2014. International Journal of Infectious Diseases, 50:75-82.
Publisher | Google Scholor - Jean, S.S., Ko, W.C., Hsueh, P.R. (2022). Global threat of carbapenem-resistant Gram-negative bacteria. Frontiers in Cellular and Infection Microbiology, 12:799508.
Publisher | Google Scholor - Karlsson, S. et al. (2019). Gender differences in sepsis: a systematic review. Critical Care, 23(1):113.
Publisher | Google Scholor - Kumarasamy, K. K., Toleman, M. A., Walsh, T. R., Bagaria, J., Butt, F., et al. (2010). Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study. The Lancet Infectious Diseases, 10(9):597-602.
Publisher | Google Scholor - Laxminarayan, R., Duse, A., Wattal, C., Zaidi, A.K., Wertheim, H.F., et al. (2013). Antibiotic resistance-the need for global solutions. The Lancet Infectious Diseases, 13(12):1057-1098.
Publisher | Google Scholor - Logan, L.K., Weinstein, R.A. (2017). The epidemiology of carbapenem-resistant Enterobacteriaceae: The impact and evolution of a global menace. Journal of Infectious Diseases, 215(Suppl_1):S28-S36.
Publisher | Google Scholor - Munoz-Price, L.S., Poirel, L., Bonomo, R.A., Schwaber, M.J., Daikos, G.L., et al. (2013). Clinical epidemiology of the global expansion of Klebsiella pneumoniae carbapenemases. The Lancet Infectious Diseases, 13(9):785-796.
Publisher | Google Scholor - Nordmann, P., Naas, T., Poirel, L. (2011). Global spread of carbapenemase-producing Enterobacteriaceae. Emerging Infectious Diseases, 17(10):1791-1798.
Publisher | Google Scholor - Olaitan, A.O., Morand, S., Rolain, J.M., (2014). Mechanisms of polymyxin resistance: acquired and intrinsic resistance in bacteria. Frontiers in Microbiology, 5:643.
Publisher | Google Scholor - Pitout, J.D.D., Laupland, K.B. (2008). Extended-spectrum β-lactamase-producing Enterobacteriaceae: an emerging public-health concern. The Lancet Infectious Diseases, 8(3):159-166.
Publisher | Google Scholor - Pitout, J.D.D., Peirano, G. (2015). The global ascendency of CTX-M-type ESBLs. Clinical Microbiology Reviews, 28(3):633-654.
Publisher | Google Scholor - Podschun, R., Ullmann, U. (1998). Klebsiella spp. as nosocomial pathogens: Epidemiology, taxonomy, typing methods, and pathogenicity factors. Clinical Microbiology Reviews, 11(4):589-603.
Publisher | Google Scholor - Sligl, W.I., Dragan, T., Smith, S.W., (2015). Nosocomial Gram-negative bacteremia in intensive care: epidemiology, resistance, and outcomes. Canadian Journal of Infectious Diseases and Medical Microbiology, 26(5):259-264.
Publisher | Google Scholor - Van Duin, D., Doi, Y. (2017). The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence, 8(4):460-469.
Publisher | Google Scholor - Vincent, J.L., Rello, J., Marshall, J., Silva, E., Anzueto, A., et al. (2009). International study of the prevalence and outcomes of infection in intensive care units. JAMA, 302(21):2323-2329.
Publisher | Google Scholor - World Health Organization. (2017). Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. Geneva: WHO.
Publisher | Google Scholor - Zankari, E., Hasman, H., Cosentino, S., Vestergaard, M., Rasmussen, S., et al. 2012. Identification of acquired antimicrobial resistance genes. Journal of Antimicrobial Chemotherapy, 67(11):2640-2644.
Publisher | Google Scholor























