

Research Article
Long Term Outcomes of UV-Treated Titanium Implants Treatment in Patients with Type 2 Diabetes Mellitus
1Assistant Professor, Department of Surgical Stomatology and Maxillofacial Surgery, Yerevan State Medical University, Yerevan, Armenia.
2Shabani Dental-Advanced General and Cosmetic Dentistry La Crescenta-Montrose, California, United States of America.
3Professor, Head of Department of Oral and Maxillofacial Surgery, Yerevan State Medical University, Yerevan, Armenia.
*Corresponding Author: Gagik Hakobyan, Professor, Head of Department of Oral and Maxillofacial Surgery, Yerevan State Medical University, Yerevan, Armenia.
Citation: Khachatryan H, Boshnaghyan E, Hakobyan G. (2026). Long Term Outcomes of UV-Treated Titanium Implants Treatment in Patients with Type 2 Diabetes Mellitus. Dentistry and Oral Health Care, BioRes Scientia Publishers. 5(1):1-8. DOI: 10.59657/2993-0863.brs.26.060
Copyright: © 2026 Gagik Hakobyan, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 04, 2026 | Accepted: March 25, 2026 | Published: April 06, 2026
Abstract
Background: The fact that the modification of the implant surface can affect the success of osseointegration has been proven in various studies. Since osseointegration efficiency is lower compared to healthy patients in diabetic patients, it is important to use surface-improved implants. The Osseo integrative properties of implants patients in diabetic patients can be improved by applying UV photo functionalization of the surface implant.
Objective: The objective of this study was to evaluate the effectiveness of prosthetic rehabilitation patients with type 2 diabetes mellitus using UV-treated titanium implants.
Methods: This is a blind randomized clinical prospective study in 73 diabetic patients with unilateral/bilateral missing teeth and final. The age of the patients ranged from 36 to 68 years; 41 men and 32 women were included. To evaluate the results, the following indicators were included: implant survival, men’s MBL, PPD, BOP, RFA, prosthetic success, quality of life. Oral health-related quality of life was assessed using the OHIP-G scale (from 1 to 5 points).
Results: During implantation and in the post-implantation period, no serious biological or prosthetic. The mean BOP, MBL, PPD showed a statistically significant difference from baseline 3 month, 6 months after 3 years (p≤0.05) in both Group A and Group B. But, BOP, MBL, PPD was found to be greater in Group-B than Group B at 3 month, 6 months and after 3 years (p≤0.05). Survival rate of implants in patients Group-A during the 3 years of functional loading 96,6%, in Group-B during the first year of functional loading 94,8%.
Conclusion: In patients diagnosed with type 2 diabetes mellitus and edentulous, with careful surgical planning and constant maintenance of normal blood glucose levels, UV-treated titanium implants can be successfully used with good results.
Keywords: type 2 diabetes mellitus; prolonged hyperglycemia; dental implant; OHIP-G scale; prosthodontic; rehabilitation; UV photo functionalization
Introduction
Rehabilitation of patients with complete and partial edentulous with the use of dental implants improves chewing function and quality of life [1,2]. The effectiveness of dental implantation is influenced by various factors; diabetes mellitus is one of the risk factors [3,4]. Prolonged hyperglycemia in diabetes often results in damage and/or dysfunction of multiple tissues and organs, causing adverse disease outcomes that include delayed wound healing, microvascular complications, impaired response to infection, and impaired bone metabolism and characterized by glycosuria, polyuria, polyphagia, and polydipsia [5-13].
Diabetes mellitus the past there has been a relative contraindication for implant placement due to an increased risk of implant failure and infection. Literature review regarding implant success in diabetic patients is controversial [14-16]. Shernoff et al. reported that in 89 patients with type 2 diabetes, failure rate was 2.2%; and after 1 year, the failure rate increased to 7.3% [17]. Morris HF et al. reported that patients with type 2 diabetes had more failures than patients without diabetes [18].
However, recent scientific publications have shown that dental implant success rates in patients with diabetes are similar to those in the general population [19-21]. Javed F. et al reported that successful osseointegration of a dental implant can be achieved in diabetic patients with good metabolic control [22]. Analysis of animal models with hyperglycemia has shown a decrease in osseointegration as untreated type 1 diabetes impairs bone healing around dental implants [23,24]. The osseointegrative properties of implants can be improved by applying the surface SLA method [25].
Recently, the surface of a titanium implant has been treated with ultraviolet (UV) light. UV photo functionalization changes the physicochemical properties of titanium implants, transforms titanium surfaces from hydrophobic to superhydrophilic [26]. UV radiation increases protein absorption and adhesion, as well as proliferation, differentiation and mineralization of osteogenic cells [27]. It is shown that the modification of the surface of the implant increases the effectiveness of dental implantation [28,29].
There are experimental studies showing the positive effect of UV-treated titanium implants in animal models [30,31]. However, there is little information in the literature on the effects of ultraviolet exposure on titanium implants used in patients with diabetes. This study assessed the effectiveness of prosthetic rehabilitation in patients with type 2 diabetes mellitus using UV-treated titanium implants.
Methodology
Study Design
This is a blind randomized clinical prospective study in 109 patients with diabetes with unilateral/bilateral missing teeth and final.
Study Population
Final sample size 73, the age of the patients ranged from 36 to 68 years, 41 men and 32 women were included.
Ethical Approval and Consent to Participate
The study was reviewed and approved by University Ethical Committee and in accordance with those of the World Medical Association and the Helsinki Declaration. Patients were informed verbally and in writing about the study and gave written informed consent.
Assortment of Subjects
The subjects selected for study were examined under the inclusion and exclusion criteria and sign the written consent. Patients were given detailed information about the methods and concepts of treatment with short implants.
Inclusion Criteria
Patients with type 2 diabetes, single or multiple missing teeth of the mandible and maxilla upper jaw, availability of space for prosthetics; residual bone height from > 8mm; horizontal residual bone of at least > 6 mm.
Exclusion Criteria
Uncontrolled oral disease, maxillary sinus disease, patients treated with corticosteroids or bisphosphonates, smokers who smoke more than 10 cigarettes per day and patients with periodontitis.
Randomization, Blinding and Treatment Allocation
The patients were divided into two groups using a computer-generated randomization:
- Group-A included 37 patients (age of the patients ranged from 36 to 68 years, 22 men and 15 women aged 36 to 67yers) were included with UV-photofunctionalized 154 implants.
- Group-B included 36 patients (age of the patients ranged from 38 to 65 years, 19 men and 17 women) were included with non-UV- photofunctionalized 148 implants.
UV functionalization of the implant surface was carried out using a UV Activator (YWJ-QSY001, Wenjian Medikal Enstriman, Foshan) for 20 seconds. Implants were placed according to standard surgical protocol. The patients underwent a thorough clinical laboratory examination according to the generally accepted scheme. The qualitative and quantitative parameters of the jaw bones of the patients were diagnosed using cone beam computed tomography (CBCT). The final diagnosis was made to the patients and a treatment option was proposed.
Criteria for Diagnosing Diabetes
Symptoms include increased thirst, increased urination, and unexplained weight loss. A random venous plasma glucose concentration ≥ 11.1 mmol/l or a fasting plasma glucose concentration ≥ 7.0 mmol/l (whole blood ≥ 6.1 mmol/l) or two-hour plasma glucose concentration ≥ 11.1 mmol/l two hours after 75g anhydrous glucose in an oral glucose tolerance test (OGTT). Blood glucose levels were monitored as recommended by the American Diabetes Association (to have an HbA1C level of less than 7% or 154 mg/dL). Implant surgery was performed after periodontal therapy. Patients underwent implantation with HbA1c levels less than 7.2% or less than 154 mg/dL.
Before implantation, all patients underwent sanitation of the oral cavity, complex periodontal treatment, extraction of hopeless teeth, treatment and filling of carious teeth, replacement of poorly fitting restorations and prostheses and complex periodontal therapy. Surgical placement of implants was performed using a 2-stage protocol using a flapless approach with digital planning with diagnostic models, ensuring the placement of the implant in the correct three-dimensional position. Due to the peculiarities of microcirculation disorders and, accordingly, tissue trophism it should be postoperative period with the dormant stage up to 3-5 months.
To assess the primary stability of implants ISQ (Implant Stability Quotient) the resonance frequency analysis (RFA) method was used during implant placement, secondary stability after the submerged healing period (after 4-5 months) using Osstell Mentor device (Osstell AB, Göteborg, Sweden). Implant stability assessed based on ISQ values low implant stability with ISQ less than 60, medium with ISQ values of 60-70, and high with ISQ values > 70.
Patients were advised to strictly follow the postoperative instructions. All patients were prescribed prophylactic antibiotic therapy (500 mg of amoxicillin and 125 mg of clavulanic acid 1 hour before surgery); and they continued to take the antibiotic after surgery (3 capsules per day for 7 days), and the day after surgery they prescribed chlorhexidine mouthwash twice a day for 30 days.
Final dental prosthetics was performed 3-5 months after using implant-supported metal-ceramic or zirconium dioxide restorations with bridge prosthetics or crowns, after prosthetic rehabilitation, CBCT image analysis was carried out. The clinical parameters of the dental implant sites were evaluated by assessing probing depth (PD), the bleeding on probing index (BOP), marginal bone level (MBL). The gingival bleeding index was performed in the study.
BOP indices were evaluated by the following criteria
- 0 - no bleeding,
- 1 - bleeding occurs no earlier than 30 seconds,
- 2 - bleeding occurs in less than 30 seconds,
- 3 - bleeding occurs when eating or brushing your teeth.
The degree of bleeding was assessed by the criteria 0.1 - 1.0 mild inflammation,
- 1 - 2.0 medium inflammation,
- 1 - 3.0 severe inflammation.
The Probing Pocket Depth (PPD) was measured with a full millimeter with a manual periodontal probe from the edge of the mucosa to the bottom of the examined pocket.
Raining of The Examiner
2 participating investigators trained on the development of the trial, case selection, measurement techniques, sample collection, data compilation sheets and their precise role in the study. These indices were measured with a universal periodontal probe (UNC 15) at 6 sites per tooth: mesiobuccal, buccal, distobuccal, distolingual, lingual, and mesiolingual at baseline, 3 months, 6 months and after 3 years.
MBL was assess by X-ray image were taken immediately (base line for comparison) 1 year, 3 years, and 5 years after implant installation, compared with values at last follow-up. Control and postoperative radiographs were compared by analyzing the mesial and distal levels of crestal bone adjacent to the implant, the mean values per implant were calculated. Oral health-related quality of life was assessed using the OHIP-G scale (from 1 to 5 points) [32].
Statistical Analysis
Statistical analyses were performed using SPSS software. Descriptive analysis (Mean ± SD for continuous and frequencies/proportion for categorical variables) were computed for all variables of interest. P-value was considered significant at less than 0.05 and less than 0.001 for highly significant results. Analyses were conducted using Excel 2013 and R software.
Results
There were no clinical and radiological examinations of serious biological or prosthetic complications, and the functional and aesthetic outcome assessed by the patients was good. A year after the functional load, 7 patients Group-A and 16 patients Group-B were found permucositis, which was stopped after local conservative therapy. 3 years after the functional load in 2 patients Group-A and 6 patients Group-B mild peri-implantitis and 2 moderate were revealed, which was stopped by local conservative therapy or bone graft therapy. The results clinical parameters ISQ (Implant Stability Quotient) (Table 1), periodontal probing depth (PPD), the bleeding on probing index (BOP), marginal bone loss (MBL)show in (Table 2).
Table 1: Average mean ISQ (Implant Stability Quotient) patients Group.
| Group | RFA ISQ (Implant Stability Quotient) | p-value | |
| After Implant Surgery | After 3-5 Months Implant Surgery | ||
| Group-A | 69.2 ISQ | 73.6 ISQ | less than 0.05 |
| Group-B | 68.7 ISQ | 71,3I SQ | less than 0.05 |
Table 2: Average mean clinical index BOP, PD, MBL in patients Group-A, B.
| Clinical Index | Time After Implant Surgery | |||
| 6 Months | After 12 Months | After 3 Years | p-Value | |
| Group-A | ||||
| BOP | 0.93 | 1.23 | 1.37 | less than 0.05 |
| PD | 1.21mm | 1.32mm | 1.98mm | less than 0.05 |
| MBL | 0.65mm | 0,84mm | 1,23mm | less than 0.05 |
| Group-B | ||||
| BOP | 1,16 | 1.84 | 2,1 | less than 0.05 |
| PD | 1.67mm | 1.79mm | 2.34mm | less than 0.05 |
| MBL | 0,87mm | 1,21 mm | 1,46 mm | less than 0.05 |
In our study, the mean BOP, MBL, PPD showed a statistically significant difference from 6 month, 12 months and after 3 years (p≤0.05) in both Group A and Group B. But, BOP, MBL, PD was found to be greater in Group-B than Group B.
Survival rate of implants in patients Group-A during the 3 years of functional loading 95,2%. Survival rate of implants in patients Group-B during the first year of functional loading 92,8%. Reasons loss of implants in patients Group-A peri-implantitis, reasons loss of implants in patients Group-B peri-implantitis and failed osseointegration.
Average Mean OHIP-G scores were (Figure 1).
- Patients rated their satisfaction with the implant at 4.8 ± 0.3,
- Satisfaction with the operation 4.6 ± 0.4,
- Satisfaction with prosthetics 4.7 ± 0.5.
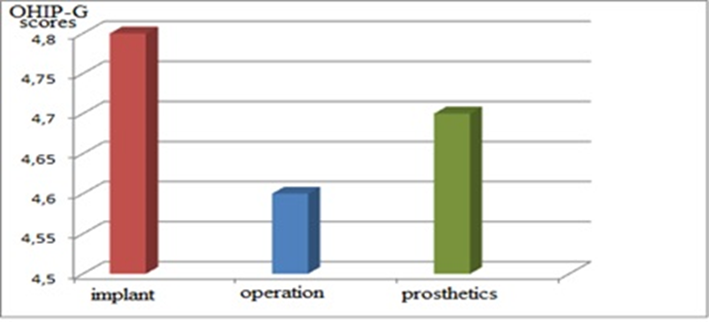
Figure 1: Oral health-related quality of life the OHIP-G scale.
After 5 years of observation occlusal function was favorable, the chewing function and aesthetics of orthopedic structures were normal. Implant failures occurred mainly after stage 2 surgery and during the first year of functional loading, which is associated with peri-implantitis (2,2%) and failed osseointegration (0.4%). In non-UV functionalized dental implants average failed osseointegration 0.3%). In UV functionalized dental implants the average failed osseointegration (0.1%). In UV functionalized dental implants average failure associated with peri-implantitis (1,5%) five-year after installation. In non-UV functionalized dental implants average failure associated with peri-implantitis (3,2%) five-year after installation.
Discussion
In recent years, the problem of diabetes mellitus has become particularly relevant due to the widespread prevalence of the disease among the world's population and the severity of complications. In diabetes mellitus, damage to various organs and systems is observed, which has many manifestations in the oral cavity [33-34]. As a result of hyperglycemia, patients become susceptible to infections and subsequent complications. It is known that during surgical interventions in patients with diabetes, wound healing time is prolonged, and recovery processes worsen due to systemic disorders of microvascular and bone metabolism, and suppression of the immune system [35-37]. Patients with diabetes also have a high rate of tooth loss due to the high prevalence of periodontal disease [38,39]. In this group of patients, tooth loss leads to disorders of the digestive system, which can also have a negative impact on the general somatic status of the patient, so it is very important to provide them with rational prosthetics in an effective and optimal manner [40,41].
In patients with diabetes mellitus, the effectiveness of treatment with removable plate dentures is low. The use of dental implants in modern dentistry greatly contributes to increasing the effectiveness of prosthetic rehabilitation in patients with type 2 diabetes [42,43]. In patients with type 2 diabetes which adversely affects wound healing and bone metabolism, immunological response, these patients are more susceptible to infections [44,45]. Hyperglycemia disrupts the osseointegration process, as decreased bone formation has a detrimental effect on the bone matrix and may have a significant impact on long-term implant survival [46]. The process of osseointegration depends not only on the level of bone tissue metabolism, but also on the state of immune homeostasis of the oral mucosa of patients [47,48]. As a consequence, the growth and accumulation of the extracellular bone matrix decreases, during healing, bone formation decreases, which can slow down the process of osseointegration [49].
The fact that modification of the implant surface can affect the success of osseointegration has been demonstrated in various studies [50,51]. Currently, to improve the process of osseointegration, various methods are used to modify the surface of titanium implants, which enhances the initial attachment of osteoblasts to the surface of the implant. UV radiation or photofunctionalization is one of the newest methods of surface modification of the implant surface. UV radiation changes the physical and chemical properties of the titanium implant surface from hydrophobic to superhydrophilic. Implant surface ultraviolet functionalization can affect osseointegration success [52-56]. UV irradiation of the surfaces of titanium implants also showed an antimicrobial effect, reducing the number of periodontal pathogenic bacteria due to increased photocatalytic properties, which can have an antimicrobial effect [57,58]. Periodontitis of varying severity occurs in most patients with diabetes, and for successful functioning of implants and prevention of peri-implantitis in patients in this category, regular maintenance of periodontal therapy is necessary and good control of blood glucose levels [59].
Monitoring stable periodontal status is a key factor in increasing long-term implant survival in diabetic patients and may provide a better prognosis. This study analyzed the long-term results of treatment of 123 patients with type 2 diabetes mellitus using dental implantation. The implant survival rate was 97.4
Conclusion
This study confirmed that implant therapy can be successfully used in patients with type 2 diabetes mellitus use of UV-treated titanium implants, with careful planning of the surgical intervention and maintaining normal blood glucose levels at all times.
Declarations
Conflict of Interest and Financial Disclosure
The author declares that he has no conflict of interest and there was no external source of funding for the present study. None of the authors have any relevant financial relationship(s) with a commercial interest.
Consent Statement
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
No.
Ethical Approval
The study was reviewed and approved by the local Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration. Informed consent Patients were informed verbally and in writing about the study and gave written informed consent.
Acknowledgements
Not applicable.
References
- Elani HW, Starr JR, Da Silva JD, Gallucci GO. (2018). Trends in Dental Implant Use in the U.S., 1999-2016, and Projections to 2026. J Dent Res. 97(13):1424-1430.
Publisher | Google Scholor - Jofre J, Castiglioni X, Lobos CA. (2013). Influence of minimally invasive implant-retained overdenture on patients' quality of life: a randomized clinical trial. Clin Oral Implants Res. 24(10):1173-1177.
Publisher | Google Scholor - Smith RA, Berger R, Dodson TB. (1992). Risk factors associated with dental implants in healthy and medically compromised patients. Int J Maxillofac Implants, 7:367-372.
Publisher | Google Scholor - Moy PK, Medina D, Shetty V, et al. (2005). Dental implant failure rates and associated risk factors. Int J Oral Maxillofac Implants, 20:569-577.
Publisher | Google Scholor - American Diabetes Association. (2021). 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care. 44(1):15-33.
Publisher | Google Scholor - Chawla A, Chawla R, Jaggi S. (2016). Microvascular and macrovascular complications in diabetes mellitus: Distinct or continuum? Indian J Endocrinol Metab. 20(4):546-551.
Publisher | Google Scholor - Sharma, A., Mittal, S., Aggarwal, R. et al. (2020). Diabetes and cardiovascular disease: inter-relation of risk factors and treatment. Futur J Pharm Sci. 6:130.
Publisher | Google Scholor - Cade WT. (2008). Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Phys Ther. 88(11):1322-1335.
Publisher | Google Scholor - Bohlen HG. (2004). Mechanisms for early microvascular injury in obesity and type II diabetes. Curr Hypertens Rep. 6(1):60-65.
Publisher | Google Scholor - Murray CE, Coleman CM. (2019). Impact of Diabetes Mellitus on Bone Health. Int J Mol Sci. 20(19):4873.
Publisher | Google Scholor - Bjornstad P, Drews KL, Caprio S, Gubitosi-Klug R, Nathan DM, et al. (2021). Long-Term Complications in Youth-Onset Type 2 Diabetes. N Engl J Med. 385(5):416-426.
Publisher | Google Scholor - Nibali L, Gkranias N, Mainas G, Di Pino A. (2022). Periodontitis and implant complications in diabetes. Periodontol 2000. 90(1):88-105.
Publisher | Google Scholor - Khader YS, Dauod AS, El-Qaderi SS, Alkafajei A, Batayha WQ. (2006). Periodontal status of diabetics compared with nondiabetics: a meta-analysis. J Diabetes Complications. 20(1):59-68.
Publisher | Google Scholor - Chrcanovic BR, Albrektsson T, Wennerberg A. (2014). Diabetes and oral implant failure: a systematic review. J Dent Res. 93(9):859-67.
Publisher | Google Scholor - Rothwell BR, Richard EL. (1984). Diabetes mellitus: medical and dental considerations. Spec Care Dentist. 4(2):58-65.
Publisher | Google Scholor - McMahon MM, Bistrian BR. (1995). Host defenses and susceptibility to infection in patients with diabetes mellitus. Infect Dis Clin North Am. 9(1):1-9.
Publisher | Google Scholor - Shernoff AF, Colwell JA, Bingham SF. (1994). Implants for type II diabetic patients: interim report. VA Implants in Diabetes Study Group. Implant Dent. 3:183-185.
Publisher | Google Scholor - Morris HF, Ochi S, Winkler S. (2000). Implant survival in patients with type 2 diabetes: placement to 36 months. Ann Periodontol. 5(1):157-165.
Publisher | Google Scholor - Michaeli E, Weinberg I, Nahlieli O. (2009). Dental implants in the diabetic patient: systemic and rehabilitative considerations. Quintessence Int. 40(8):639-645.
Publisher | Google Scholor - Alzahrani AS, Abed HH. (2016). To what extent should dental implant placement be adopted as a standard for diabetic patients? Saudi Med J. 37(11):1179-1183.
Publisher | Google Scholor - Oates TW, Huynh-Ba G, Vargas A, Alexander P, Feine J. (2013). A critical review of diabetes, glycemic control, and dental implant therapy. Clin Oral Implants Res. 24(2):117-127.
Publisher | Google Scholor - Javed F, Romanos GE. (2009). Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: a systematic literature review. J Periodontol. 80(11):1719-1730.
Publisher | Google Scholor - Siqueira JT, Cavalher-Machado SC, Arana-Chavez VE, Sannomiya P. (2003). Bone formation around titanium implants in the rat tibia: role of insulin. Implant Dent. 12(3):242-251.
Publisher | Google Scholor - de Molon RS, Morais-Camilo JA, Verzola MH, Faeda RS, Pepato MT, et al. (2013). Impact of diabetes mellitus and metabolic control on bone healing around osseointegrated implants: removal torque and histomorphometric analysis in rats. Clin Oral Implants Res. 24(7):831-837.
Publisher | Google Scholor - Khandelwal N, Oates TW, Vargas A, et al. (2013). Conventional SLA and chemically modified SLA implants in patients with poorly controlled type 2 diabetes mellitus-a randomized controlled trial. Clin Oral Implants Res. 24:13-19.
Publisher | Google Scholor - Flanagan D. (2016). Photofunctionalization of Dental Implants. J Oral Implantol. 42(5):445-450.
Publisher | Google Scholor - Lee JB, Jo YH, Choi JY, Seol YJ, Lee YM, et al. (2019). The Effect of Ultraviolet Photofunctionalization on a Titanium Dental Implant with Machined Surface: An In Vitro and In Vivo Study. Materials (Basel). 12(13):2078.
Publisher | Google Scholor - Khachatryan H, Hakobyan G. (2023). Diagnostic and prognostic value of indicators of markers of bone metabolism in type 2 diabetes mellitus patients with UV functionalised dental implants. J Stomatol Oral Maxillofac Surg. 124(6S):101608.
Publisher | Google Scholor - Ghambaryan N, Yessayan L, Hakobyan G. (2024). Long-term effectiveness of UV functionalised short (≤ 6 mm) dental implants placed in the posterior segments of the atrophied maxilla: controlled case series. Odontology.
Publisher | Google Scholor - Jin S, Yamamoto Y, Harada Y, Kaneko S, Oishi K, et al. (2022). Effectiveness of photofunctionalized titanium alloy on osseointegration in rats with type 2 diabetes. J Orthop Surg Res. 17(1):445.
Publisher | Google Scholor - Akiyoshi FUNATO, Shinichi KOMATSU, Hisato HOTTA, SUGITA, Akira WADA, Kazuo TAKEUCHI, et al. (2019). An Investigation of Osteogenesis on Ultraviolet Light-treated Surfaces Using a Type 2 Diabetes Rat Model. Journal of Japanese Society of Oral Implantology. 339-345.
Publisher | Google Scholor - John MT, Patrick DL, Slade GD. (2002). The German version of the Oral Health Impact Profile--translation and psychometric properties. Eur J Oral Sci. 110(6):425-433.
Publisher | Google Scholor - American Diabetes Association. (2017). 2. Classification and diagnosis of diabetes. Diabetes Care. 40(1):S11-S24.
Publisher | Google Scholor - Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, et al. (2019). Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 157:107843.
Publisher | Google Scholor - Cade WT. (2008). Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Phys Ther. 88(11):1322-1335.
Publisher | Google Scholor - Murray CE, Coleman CM. (2019). Impact of Diabetes Mellitus on Bone Health. Int J Mol Sci. 20(19):4873.
Publisher | Google Scholor - Chawla A, Chawla R, Jaggi S. (2016). Microvasular and macrovascular complications in diabetes mellitus: Distinct or continuum? Indian J Endocrinol Metab. 20(4):546-551.
Publisher | Google Scholor - Lalla E, Papapanou P. (2011). Diabetes mellitus and periodontitis: a tale of two common interrated diseases, Nat Rev Endocrinol, 7(12):738-748.
Publisher | Google Scholor - Saremi A, Nelson RG, Tulloch-Reid M, et al., (2005). Periodontal disease and mortality in Type 2 diabetes, Diab Care, 28:27-32.
Publisher | Google Scholor - Patel MH, Kumar JV, Moss ME. (2013). Diabetes and tooth loss: an analysis of data from the National Health and nutrition examination survey, 2003-2004. J Am Dent Assoc. 144(5):478-485.
Publisher | Google Scholor - Hastings JF, Vasquez E. (2017). Diabetes and tooth loss among working-age African Americans: a national perspective. Social Work in Public Health. 32(7):443-445.
Publisher | Google Scholor - Al Ansari Y, Shahwan H, Chrcanovic BR. (2022). Diabetes Mellitus and Dental Implants: A Systematic Review and Meta-Analysis. Materials (Basel). 29;15(9):3227.
Publisher | Google Scholor - Fazard P, Andersson L, Nyberg J. (2002). Dental implant treatment in diabetic patients. Implant Dent, 11:262-267.
Publisher | Google Scholor - Dasari N, Jiang A, Skochdopole A, Chung J, Reece EM, et al. (2021). Updates in Diabetic Wound Healing, Inflammation, and Scarring. Semin Plast Surg. 35(3):153-158.
Publisher | Google Scholor - Murray CE, Coleman CM. (2019). Impact of Diabetes Mellitus on Bone Health. Int J Mol Sci. 20(19):4873.
Publisher | Google Scholor - Wang X, Wang H, Zhang T, Cai L, Kong C, et al. (2020). Current Knowledge Regarding the Interaction Between Oral Bone Metabolic Disorders and Diabetes Mellitus. Front Endocrinol (Lausanne). 11:536.
Publisher | Google Scholor - Dubey RK, Gupta DK, Singh AK. (2013). Dental implant survival in diabetic patients; review and recommendations. Natl J Maxillofac Surg. 4(2):142-150.
Publisher | Google Scholor - Zhou W, Tangl S, Reich KM, Kirchweger F, Liu Z, et al. (2019). The Influence of Type 2 Diabetes Mellitus on the Osseointegration of Titanium Implants with Different Surface Modifications-A Histomorphometric Study in High-Fat Diet/Low-Dose Streptozotocin-Treated Rats. Implant Dent. 28(1):11-19.
Publisher | Google Scholor - Ma, Y., Wang, S., Wang, H. et al. (2023). Mesenchymal stem cells and dental implant osseointegration during aging: from mechanisms to therapy. Stem Cell Res Ther. 14:382.
Publisher | Google Scholor - Smeets R, Stadlinger B, Schwarz F, Beck-Broichsitter B, Jung O, et al. (2016). Impact of Dental Implant Surface Modifications on Osseointegration. Biomed Res Int. 6285620.
Publisher | Google Scholor - Kligman S, Ren Z, Chung C-H, Perillo MA, Chang Y-C, et al. (2021). The Impact of Dental Implant Surface Modifications on Osseointegration and Biofilm Formation. Journal of Clinical Medicine. 10(8):1641.
Publisher | Google Scholor - Houshmand B, Rezaei Esfahroodi Z, Behnamghader A, Mohammadreza S, Azizi A, et al. (2023). Evaluation of UV photofunctionalization effect on ultrastructural properties of SLA titanium disks: An in vitro study. J Adv Periodontol Implant Dent. 15(2):117-122.
Publisher | Google Scholor - Chang LC. (2022). Clinical Applications of Photofunctionalization on Dental Implant Surfaces: A Narrative Review. J Clin Med. 11(19):5823.
Publisher | Google Scholor - Minamikawa H., Ikeda T., Att W., Hagiwara Y., Hirota M., et al. (2014). Photofunctionalization increases the bioactivity and osteoconductivity of the titanium alloy Ti6Al4V. J. Biomed. Mater. Res. A. 102:3618-3630.
Publisher | Google Scholor - Aita H, Hori N, Takeuchi M, Suzuki T, Yamada M, et al (2009). The effect of ultraviolet functionalization of titanium on integration with bone. Biomaterials. 30:1015-1025.
Publisher | Google Scholor - Jun JH, Oh KC, Park KH, Jung N, Li J, et al. (2021). Improvement of osseointegration by ultraviolet and/or simvastatin treatment on titanium implants with or without bone graft materials. Materials. 14(13):3707.
Publisher | Google Scholor - Yamada Y., Yamada M., Ueda T., Sakurai K. (2014). Reduction of biofilm formation on titanium surface with ultraviolet-C pre-irradiation. J. BioMater. Appl. 29:161-171.
Publisher | Google Scholor - de Avila E.D., Lima B.P., Sekiya T., Torii Y., Ogawa T., et al. (2015). Effect of UV-photofunctionalization on oral bacterial attachment and biofilm formation to titanium implant material. Biomaterials. 67:84-92.
Publisher | Google Scholor - Nourah D, Aldahlawi S, Andreana S. (2022). Should the Quality of Glycemic Control Guide Dental Implant Therapy in Patients with Diabetes? Focus on Implant Survival. Curr Diabetes Rev. 18(4):e060821195367.
Publisher | Google Scholor























