

Review Article
Female Genital Mutilation and The Risk of Genital Cancers: A Clinical Perspective
Department of Biotechnology, Savitribai Phule Pune University, Pune, Maharashtra, India.
*Corresponding Author: Rajesh Nivarti Gacche, Department of Biotechnology, Savitribai Phule Pune University, Pune, Maharashtra, India.
Citation: Gacche RN. (2026). Female Genital Mutilation and The Risk of Genital Cancers: A Clinical Perspective, Journal of Women Health Care and Gynecology, BioRes Scientia Publishers. 6(1):1-14. DOI: 10.59657/2993-0871.brs.26.107
Copyright: © 2026 Rajesh Nivarti Gacche, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 12, 2026 | Accepted: March 31, 2026 | Published: April 09, 2026
Abstract
Female genital mutilation (FGM) remains a major global health concern, affecting more than 230 million girls and women worldwide according to UNICEF’s 2024 report. Despite the absence of any medical or therapeutic justification, FGM persists across numerous regions and is associated with a wide spectrum of physical, obstetric, and psychological harms. While its acute and short-term health consequences are well documented, the long-term sequelae particularly its potential contribution to genital carcinogenesis remain insufficiently explored. FGM induces a range of physiological and pathophysiological alterations, including genital tissue injury, chronic inflammation, scarring and keloid formation, disruptions in tissue repair and regeneration, and increased susceptibility to high-risk human papillomavirus (HPV) infection. These factors collectively may create a microenvironment conducive to the development of cervical, vulvar, and vaginal malignancies. This review synthesizes current global clinical evidence on FGM and examines emerging mechanistic pathways that may link FGM to an elevated risk of genital dysplasia and cancer. Although the World Health Organization and the World Medical Association have denounced FGM as a violation of human rights, progress toward its global elimination remains slow. A deeper understanding of its potential carcinogenic implications may provide critical insights to strengthen public health interventions and intensify global advocacy for the eradication of this harmful practice.
Keywords: FGM; oncogenesis; genital cancers; FGM induced pathophysiology and cancer risk
Introduction
Female genital mutilation (FGM) or cutting is a patriarchal, oppressive, traditional, non-medical sociocultural ingrained practice that has been claimed for the control of sexual identities/chastity and bodies of women and girls. World Health Organization (WHO) defines FGM as “procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons” [1]. The recent UNICEF data highlight that over 230 million girls and women across the globe have experienced FGM and surprisingly this accounts for 15% increase in FGM cases as compared to the data which was published eight years ago [2]. The largest number of FGM cases have been observed in African countries (over 144 million cases), followed by Asia (over 80 million cases) and Middle East (over 6 million cases). Nevertheless, FGM is also practiced in diasporas around the world and in small, remote communities [2]. A cursory look at the countrywide burden of FGM (Figure 1) clearly underscore the need of collective efforts for its alleviation.
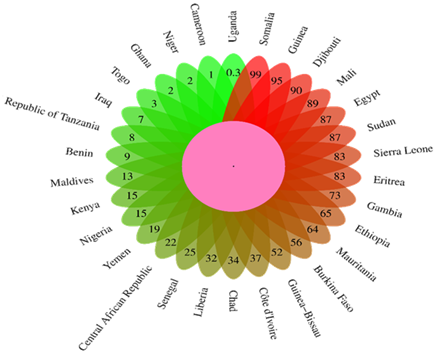
Figure 1: Global Prevalence of FGM: Proportion of females aged 15 to 49 years who have experienced FGM [2].
The FGM, being devoid of any therapeutic and medical rationale is associated with several adverse health effects, such as infection, excessive bleeding, painful urological complications, development of scars like keloids, haemorrhage, persistent inflammation, cervical dysplasia, impairment in sexual functions, etc. [3-5]. Genital harm has profound impact on women’s obstetric and gynaecological health. This reality is strongly supported by the literature which consistently highlights serious obstetric outcomes in women who have undergone FGM including postpartum haemorrhage, episiotomy, risk of delivery by caesarean section, infant resuscitation, and inpatient perinatal death etc. [6]. A women’s fortitude is not solely measured by physical strength, but equally by the resilience of her mind, which upholds the emotional and social balance of her entire family. The consequences of FGM ripple through every aspect of her health and dignity, eroding both body and mind. Accordingly, the body of research has documented numerous adverse mental health complications associated with FGM, including anxiety, posttraumatic stress disorder, depression, neuroses, and psychoses [7]. A more sobering and data rich noteworthy report reveals that, over the span of a decade-long study spanning 15 FGM practicing countries, a 50% increase in the number of girls subjected to FGM increases is associated with a 0.075 percentage point increase in their five-year mortality rate. On the surface, this fractional increment seems to be modest; but when extrapolated across these nations, this fractional elevated mortality rate translates into an alarming estimate of over 44,320 FGM-associated excess deaths every year across these countries [8].
In fact, there are different non-medical procedures employed during FGM, including the genital area being stitched shut, the removal of flesh, minor cuts without flesh removal, and other unclassified types, or instances where the type is not known or is missing. WHO has classed FGM into four major types (Figure 2), in Type 1 (clitoridectomy) there is the partial or complete removal of the clitoral glans (in fact clitoris happens to be the sensitive part of the female genitals). This type also involves the cutting of the fold of skin around the clitoral glans (the prepuce/clitoral hood). Type 2, also called as excision, wherein there is partial or complete removal of the clitoral glans and the inner folds of the vulva (labia minora), along with or without removal of the labia majora which happens to be the outer folds of skin of the vulva. In Type III, also known as infibulation, the vaginal opening is narrowed by creating a covering seal. This is achieved by cutting and repositioning either the labia minora or labia majora. The procedure may also involve the removal of the clitoral prepuce or hood, as well as the glans, but this is not always the case. Type 4 encompasses all other damaging practices such as piercing, cutting, scraping, and burning the genital area, even it also includes the non-identifiable/undisclosed practices affecting the female genitalia for non-medical reasons [1].
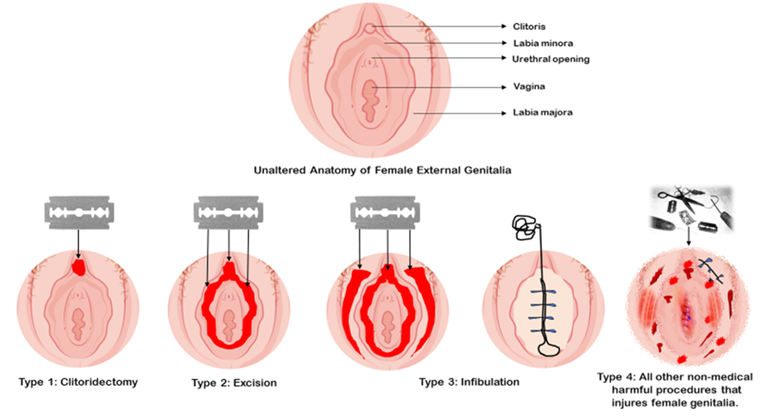
Figure 2: Different types non-medical procedures employed during FGM.
Pathophysiological Mechanisms Linking FGM to Cancer Risk: Long Lasting Impact of Genital Wound Healing and Inflammation
The intricate pathophysiological processes that interlink the FGM to a heightened cancer risk are both subtle and complex, intertwining the FGM induced psychological trauma with the gradual disruption of cellular redox balance leads to oxidative stress, which has been identified as one of the key contributors to cancer initiation [9]. Similar to an ailment that grows unnoticed, the healing and scar tissue formation from infibulation or excision disturb the fragile structure of the genital region, preparing the conducive niche for precancerous changes and genetic instability [10]. In essence, FGM acts as a covert precursor, a quiet and ongoing violence that imprints itself not only the physical body but also on the cellular architecture of the affected tissues, creating an environment that encourages the unchecked growth of abnormal cells which might take a cancerous route. The fact that cutting of nerve endings and the remodeling of tissue architectures leads to chronic inflammation, which is known to generate reactive oxygen species (ROS), release pro-cancerous cytokines/growth factors involved in suppression of anti-tumour immune response [11]. Therefore, the physical process of FGM represents only the silent surface of a deeper concealed malady, wherein the more dangerous and inscrutable series of cellular underpinnings that lurk beneath, sabotaging tissue integrity and elevating the long-term risk of genital cancers particularly the squamous cell carcinoma of the vagina, vulva and cervix [5]. In many ways, this silent yet significant insidious modification of the body mirrors and set the narrative of cancer itself, where seemingly minor events whether a mutation, or inflammatory response, HPV infection or a shift in cellular disposition can trigger and may recruit the calamitous events leading to deadly malignancy [12].
Nevertheless, more seriously reported fact is that FGM has been implicated in heightening the susceptibility to HIV infection through series of biological and contextual mechanisms. As the FGM is frequently performed using non-sterile tools and under conditions that disregard even the basic hygiene practices, the open wounds with torn mucosa, lack of protective epithelial shield may provide invitation for HIV entry and transmission [13].
How FGM Induced Genital Scarring/ Keloids May Prime the Tissues for Oncogenesis
One of the most adverse and perilous outcomes of FGM is the development of scars which essentially develops as remnants of trauma and suffering. The inscrutable link between FGM induced scarring and risk of oncogenesis is not merely a matter of anatomy remodeling, but a kind of cellular memory deeply imprinted into the tissue long after the ritual of FGM has been faded into silence. Besides genital skin cells display a more delicate, volatile and dynamic immune response compared to other sites, there also exists biochemical distinctions between genital and non-genital skin, for example the dermal elastin content around 2 to 8%, while genital skin comprises of up to 29% elastin. Of note, skin adjacent to the outer genitalia are more susceptible to excessive scarring [14]. Perhaps scarring is a cruel twist, for a region that experienced so much of adversities and demonstrates so little of what it has faced.
Before we discuss the risk of FGM induced scarring and its association with initiation of cancer, there is need to understand pathophysiology of scarring. There are two categories of pathological scarring after physical injury. The one is called as hypertrophic scars, while the other is keloids. In the process of wound healing, hypertrophic scars originate after trauma, surgery, burns, or even spontaneously in susceptible patients. As compared to hypertrophic scars, keloids behave differently and invade beyond the margins of the original tissue damage area, rarely regress and are strongly influenced by genetic factors. From histology point of view hypertrophic scars and keloids consists of diverse architecture arrangement of collagen fibres, presence of α-smooth muscle actin positive myofibroblasts, and the degree of angiogenesis [15]. Keloids, the stubborn fibrous outgrowths of scar tissue are ensnared in a loop of unceasing inflammation, a cycle that fails to cease and there lies the subdued, yet inexorable role of persistent inflammation quietly shaping the conditions and creating niche for the onset of oncogenesis.
The key molecular pathways, such as PI3K/AKT, TGF-β/Smad, JAK/STAT, and MAPK are the major signaling players involved in pathophysiology of keloid formation, where they drive cellular processes like proliferation of fibroblast, relentless synthesis of collagen, and extensive deposition of extracellular matrix. Yet it is precisely, the same molecular conduits, which are frequently implicated in the dysregulation of cellular processes that contribute to malignancy [16]. Therefore, keloids are considered as benign fibroproliferative dermal tumours owing to their cancer-like mimics such as progressive uncontrolled growth, lack of spontaneous regression and significantly high rates of recurrence [11,17]. Nevertheless, in a comprehensive population-based systematic study involving 17,401 individuals diagnosed with keloids, a striking trend of overall 1.49-fold higher cancer risk was observed in keloids patient group as compared to control population group [18].
So now we must ask a question, whether scars and keloids emerge in the aftermath of FGM procedures? and if yes, do they have any association with onset of oncogenesis in FGM survivors? Clearly, the answer to both questions is cautiously affirmative and there exists a positive correlative discourse in the current clinical literature. In fact, the development of keloids has been observed as a known complication after commission of FGM [4], and unfortunately tend to be recurrent as well [19]. To address the first question with clinical reality, in a retrospective study of 27 patients with a history of undergoing FGM, all participants were presented with clitoral masses and each patient was pre-diagnosed with clitoral keloid. This suggests a strong clinical association between FGM induced keloid formation at the site of genital cutting [20]. A community-based survey conducted in rural Gambia to assess the long-term reproductive health consequences of FGM observed excessive keloid formation as one of the most commonly cited negative consequences of FGM [21]. Notably, the research has observed that the individuals with a deeper melanin hue in their skin are more susceptible to developing keloids as compared to those with light-skin tones [22].
In fact, FGM is cloaked in silence, not by accident, but by barbaric design. It’s operated in private spheres, concealed by cultural taboos and in the realm of unspoken code of secrecy that stifles conversation and suppresses reporting of both its commission and consequences. As a result, the clinical registry of its adverse outcomes remains obscure, hidden, and often suppressed in public domain. Although the direct clinical causal evidence is still emerging, however the prevailing clinical and pathophysiological scientific discourse strongly supports a cautiously affirmative link between FGM-induced keloids and the potential onset of oncogenesis. In fact, it is imperative to regard this as a solemn warning, not shouted but quietly acknowledged that the formidable keloid scars, born of violence, may harbor a latent risk turning hostile and recruiting genital malignancy in FGM survivors [17,18,23-25].
FGM induced Cervical Dysplasia and Cervical Cancer: Early Pathophysiological Changes Leading to Malignancy
In the intricate tapestry of women's health who are victims of genital mutilation, clinical evidence links FGM with cervical dysplasia (CD): a precancerous affliction, that silently mark the cervix as a site of possible malignancy. Given the precancerous nature of CD and its inherent risk of progression into invasive cervical cancer, there is a compelling need for the continual development of innovative diagnostic and therapeutic modalities for effective management of CD [26]. Dysplasia, a term that might, prima facie sounds somewhat benign, literally means “disordered growth” and in medical terminology it is called as cervical intra-epithelial neoplasia. This disorder is curable but if left untreated, it may eventually develop into invasive cervical cancer. There are at least 448 types of HPV reported out of which 15 stains have been classified as carcinogenic. Persistent and pernicious infection of mostly HPV 16 and 18 has been implicated as principal culprit in the causation of CD and cervical cancer [27]. In addition to HPV infection, other non-infectious factors such as smoking, levels of micronutrients, oral contraceptives, sexual behaviour, chronic infections and inflammations have also been attributed in the development of CD [28]. In a curious turn of fate, interestingly, the infection of Fusobacterium species whose role in the onset of CD was once unknown, now linked in the development of CD [29].
In the pathogenesis of HPV mediated cervical cancer, initially HPV invade and infects the basal cells of the squamous epithelium of the cervical region. Once entered in the host cell, the HPV DNA replicates in coordination with the basal cells as they differentiate and migrate towards the surface of the epithelium. During the process of persistent infection, HPV gene expression becomes dysregulated and no longer inked to the state of cellular differentiation. This dysregulation leads to aberrant overexpression of early viral oncoproteins E6 and E7. The E6 protein facilitates the degradation of tumour suppressor p53 protein, while E7 mediates the inactivation of pRb, both are key proteins involved in regulating the cell cycle. The loss of this regulatory pathway leads to loss of cell cycle control and genomic stability. The infected epithelial cells develop abnormal morphologic features, including immature basaloid-type squamous cells and mitotic figures extend in the upper layers of the cervical epithelium [30]. This tragedy unfolding in the cervix marks the beginning of a silent, insidious threat of cervical cancer if left untreated.
The Incidence of Cervical Dysplasia/Cancer in Women with FGM: Insights from Clinical and Epidemiological Studies
In fact, the clinical connection of FGM induced CD or cervical cancer is an uncharted territory and yet to be established on scientific grounds. Even with FGM type III (infibulation) wherein the cutting and repositioning either the labia minora or labia majora is performed, the clear clinical evidence is lacking, however the cursory glance at the recently accumulated literature reveals that FGM serve as an accelerant risk factor that might exacerbate the pathways towards development of CD and over time, the stealthy development of cervical cancer. Series of clinical reports and systematic reviews involving clinical studies have shown that the girls and women who are exposed to FGM are at greater risk for developing genitourinary health problems including CD and cervical cancer [31-34].
In a retrospective study tracing the medical history of the refugee women over six years, there was strong association (36.8%) of HPV infection and CD. Quietly, another detail surfaced, wherein the FGM was associated with higher rate of dysplasia (11.3%) amongst the FGM experienced women, however the outcome was not statistically conclusive [34]. Migrant women who have undergone type III FGM might be at more risk for development of cervical dysplasia. In line with this concern, a descriptive retrospective cross-sectional study conducted at specialized clinic in Switzerland was specifically designed to assess the prevalence of CD among migrant women with FGM, the study illuminated an adverse obstetric outcome and a grim correlation between FGM and CD. The study involved in assessment of 338 medical records, and troubling figure emerged with prevalence of high-grade squamous intraepithelial lesions or worse among the migrant women with FGM was 2.95%, a number almost fivefold observed in the general Swiss women population (0.58%). Notably, in this thematically resonant inquiry, most of the FGM women were from Eritrea and Somalia (60.4%) having 55.6% of FGM type III [32]. In yet another retrospective cross-sectional setting conducted at Geneva University Hospitals reviewing medical records (2010-2016) of 188 women with type III FGM, CD was observed in 10.6% of cases, along with 8.5% having low-grade lesions or HPV-positive atypical squamous cells of undetermined significance, and 2.1% with high-grade lesions, including one alarming case of carcinoma in situ also called as stage 0 cancer [35]. FGM remains concealed in silence, deliberately it is escaped from hospital registries, owing to cultural complicity burden, institutional discomfort and the weight of inherited silence. FGM victimized women also think that documenting FGM in public domain is a kind of betrayal of community norms and customs. In short, genital mutilated women’s body bears the mark, but the paper remains blank, this is not because the wound is invisible, but because acknowledging the commission of FGM may invite legal action, accountability, and change. For example, in Switzerland and Belgium, it is difficult to project the real prevalence of cervical dysplasia or cancer because over 30% of all eligible women refrain from participating in cervical cancer screening and prevention for several reasons [36]. Therefore, the number of clinical reports exposing the link between FGM and CD or cervical cancer unfolds slowly. But besides that, the current findings remind us that scars of FGM have incipient potential of transforming the affected tissues into malignancies long after the commission of FGM and one of the major culprits could be FGM especially type III for the onset of CD and cervical cancer [37].
The Blade’s Cut That Echoes: How FGM induced Genital Anatomical Disruptions Opens the Door to HPV- The Silent Herald of Cervical Cancer
In the labyrinth of medical corridors, where scientific truths are often shrouded in enigma, one of the most significant breakthroughs in the mainstream of cancer research was the identification of persistent infection with certain genotypes that drives the cervical cancer. Since then, the scientific community has developed range of diagnostic and therapeutic modalities for the effective management of cervical cancer. Significant advances have been made in understanding the molecular underpinnings of HPV induced pathogenesis leading to cervical cancer [27]. One of the most notable features of HPV pathogenesis is that it does not storm the gates but waits for a fracture in the fortress. It slips quietly into the deepest layer of the epithelium through the damaged tissue, which eventually allows it to establish a crosstalk with the cells of the basal layer of the epidermis. FGM by its very intent, orchestrates breach in genital anatomical integrity and thereby creates a vulnerable niche for the entry and establishment of HPV [38]. While probing the pathophysiology of cervical cancer, one has to understand the fact that HPV is a necessary but not sufficient cause of cervical cancer, this clearly indicates the role of inscrutable players especially related to tissue damage and inflammation [39].
In the most disquieting realm of clinical observations, it has been noted that women who have suffered the indignity of FGM, exhibit higher incidence of HPV infections that foul contagion which often leads to cervical cancer. For example, Nigeria a country embraced with hard hands of traditions and customs accounts for nearly a quarter of global cases of FGM. In a study designed to investigate the relationship between FGM undergone women and prevalence of HPV infection observed over 11.5% positive participants for one or other strain of HPV. The observation worth of noting is over 78.3% of HPV positive cases were observed among FGM women. Perhaps the more alarming was the diversity of high-risk HPV viral genotypes detected, wherein over seventeen different types were diagnosed in FGM subjects, including the most carcinogenic HPV 16, 18 and other 9 high-risk strains. The statistics did not flinch, and showed cruel correlation (p=0.0052, 95% CI) between FGM and HPV infection. More seriously, the outcome of this study also documented a case of quintuple HPV infection in a single individual in Nigeria [40]. Additional reports also resonate similar trend of detecting series of high-risk HPV genotypic variants from abnormal cervical smears. Notably, the cases of multiple HPV infections appear to be more prevalent in women who have undergone FGM, suggesting that the FGM induced injury creates a niche conducive to harboring diverse HPV strains [41,42].
In the quest of disentangling the unfathomable intricate threads connecting FGM, cervical cancer, and HPV infection, a retrospective study conducted in Senegal: a country located on the west coast of Africa, has illuminated a strikingly closer association FGM and onset of invasive cervical cancer. The analysis of over 2,398 medical records of women aged 18-90 years from Dakar, Senegal revealed that there exists a strong correlation between FGM and invasive cervical cancer (95% CI). In addition, the outcome of the study also observed that the risk of invasive cervical cancer was significantly amplified in FGM women who were HPV-positive, clearly suggesting that FGM could be a critical cofactor in the pathogenesis of cervical cancer in FGM women [5]. In the similar line, a study conducted in Mali, a landlocked country in West Africa with an FGM prevalence of 89%, scrutinized several FGM associated risk factors and found that women with FGM had 1.29 greater odds of developing cervical cancer [43]. WHO has identified over 144 million cases of FGM cases in African countries, a number that echoes not just in epidemiological concern but also as a wakeup call for advocacy groups exposing the exacerbated incidence of HPV infections and possible onset of cervical cancer among FGM women.
Amid the matrix of socio-demographic factors, ethnic origin and the practice of FGM intersects with onset of HPV infections. For example, the study designed to investigate the risk factors, prevalence, and HPV induced squamous intraepithelial lesions in a random cohort of women from a rural community in Gambia, clear ethnic disparity was observed in relation HPV infection and FGM. It was observed that the ethnic communities like Mandinka and Fula where FGM remains embedded as a cultural identity were identified with higher risk of 14% and 21
Conclusion
It has been poignantly expressed in Kurdish proverb: “A women’s strength is her silence, but her silence is also her suffering”. In many ways, this sentiment encapsulates the long shadow cast of FGM which affected over 230 million women and girls across the world. While its cultural underpinnings are deeply rooted in communities, but its long-term health effects, particularly its potential implications in genital carcinogenesis remain an unexplored frontier. This review has thoughtfully explored the possible link between FGM and its implications in onset of genital malignancies. Amongst the several health related concerns of FGM-induced pathophysiological processes that may contribute in the development of genital cancer, a scientific discourse has been presented here with a major emphasis of how FGM-induced genital scarring/keloids may prime the cervical tissues for oncogenesis, how it is involved in development of cervical dysplasia and a conducive niche permissive to cervical cancer, how FGM-induced genital anatomical disruptions facilitate the entry of HPV, which happens to be an established etiological agent in cervical carcinogenesis. In the final inquiry, the comparative picture of global HPV prevalence in concert with FGM practicing and non-practicing countries has been presented.
The contemporary research suggests that females who have undergone FGM are at a greater risk for developing genitourinary health complications including cervical dysplasia and cancer. The women who have experienced FGM often found to present clitoral masses and diagnosed with clitoral keloids, a type of scars that emerge after the FGM commission. Notably, individuals diagnosed with keloids have higher risk of developing genital cancer. Clinical observations also documented that FGM distorts the anatomical integrity of female genitalia. These anatomical disruptions appear to facilitate the HPV entry persistence, pinpointing the FGM as significant cofactor in the pathophysiology of cervical cancer. Several clinical reports noted that women who have suffered the indignity of FGM, have exhibited higher incidence of HPV infections as compared to non FGM subjects. Moreover, it has also been observed that countries who have FGM as a cultural practice, especially Sub-Saharan African countries in general have more prevalence of HPV infections, as compared to Nations where FGM is rare or not practiced. Every concern discussed herein is grounded in direct or indirect clinical observations. Though the threads of evidence are not yet woven into a concrete mechanistic cause-and-effect framework, still they are compelling and invites scientific curiosity. There is an urgent need for conducting both societal and clinical research that specifically examines the underlying mechanistic link between FGM and genital cancer. While the body of literature on this important issue is gradually expanding, and continues to alarm the situation quietly and persistently, positioning the practice of FGM as a potential contributing factor in the onset of genital cancer.
Despite the great strides of efforts made by international agencies (WHO, UNISEF, UNFPA, UNHRC, FIGO etc.), and global NGOs & advocacy organizations (28 Too Many, Equality Now, End FGM European Network, The Girl Generation, FORWARD, Orchid, etc.) the practice of FGM seems to be more entrenched and there is no substantial reduction in the eradication of this unethical, unlawful and deeply rooted cultural practice in many parts (mostly African) across the word. To accelerate the global efforts against FGM, an integrated and multifaceted approach is essential. Strengthening the issues like legislative and policy reforms, introducing community driven education especially at school level. Additionally, enhancing National health care system, leveraging media and technology for effective awareness campaigns, fostering sustained international collaborations and targeted fund raising etc. can collectively support a global movement against this insidious practice. This review might serve as a reference for international agencies and NGOs & advocacy groups to emphasize the adverse health outcomes of FGM and strengthen efforts towards its abolition.
Declarations
Acknowledgement
Author acknowledges the internet facility provided by the Savitribai Phule Pune University (SPPU) and the financial assistance from ANRF (File No. EEQ/2023/000151) and RUSA Phase 2 grant of SPPU Pune (MS), India.
Ethical Considerations
This review article adheres to established ethical standards for academic scholarship. As it is based solely on previously published literature and involves no original data collection or interaction with human participants, institutional ethical approval was not required. All sources have been properly acknowledged, and referenced studies are cited to ensure accurate attribution of ideas and findings.
Conflict of Interest
Author declares no conflict of interest.
Funding or Financial Support
This review article did not receive financial support from any public, commercial, or non-profit funding agency.
References
- World Health Organization. (2025). Female Genital Mutilation.
Publisher | Google Scholor - United Nations Children’s Fund. (2024). Female Genital Mutilation: A Global Concern. New York: UNICEF.
Publisher | Google Scholor - Berg, R. C., Underland, V., Odgaard-Jensen, J., Fretheim, A., Vist, G. E. (2014). Effects of female genital cutting on physical health outcomes: a systematic review and meta-analysis. BMJ Open, 4(11):e006316.
Publisher | Google Scholor - Sigurjonsson H, Jordal M. (2018). Addressing female genital mutilation/cutting (FGM/C) in the era of clitoral reconstruction: plastic surgery. Curr Sex Health Rep. 10(2):50-56.
Publisher | Google Scholor - Osterman AL, Winer RL, Gottlieb GS, et al. (2019). Female genital mutilation and noninvasive cervical abnormalities and invasive cervical cancer in Senegal, West Africa: a retrospective study. Int J Cancer. 144(6):1302-1312.
Publisher | Google Scholor - Banks, E., Meirik, O., Farley, T., Akande, O., Bathija, H., et al. (2006). Female genital mutilation and obstetric outcome: WHO collaborative prospective study in six African countries. Lancet (London, England), 367(9525):1835-1841.
Publisher | Google Scholor - Abdalla SM, Galea S. (2019). Is female genital mutilation/cutting associated with adverse mental health consequences? A systematic review of the evidence. BMJ Glob Health. 4(4):e001553.
Publisher | Google Scholor - Ghosh A, Flowe H, Rockey J. (2023). Estimating excess mortality due to female genital mutilation. Sci Rep. 13(1):13328.
Publisher | Google Scholor - Hayes JD, Dinkova-Kostova AT, Tew KD. (2020). Oxidative stress in cancer. Cancer Cell. 38(2):167-197.
Publisher | Google Scholor - Cangkrama M, Wietecha M, Werner S. (2020). Wound repair, scar formation, and cancer: converging on activin. Trends Mol Med. 26(12):1107-1117.
Publisher | Google Scholor - Coussens LM, Werb Z. (2002). Inflammation and cancer. Nature. 420(6917):860-867.
Publisher | Google Scholor - Fernandes JV, de Medeiros Fernandes TA, et al. (2015). Link between chronic inflammation and human papillomavirus-induced carcinogenesis. Oncol Lett. 9(3):1015-1024.
Publisher | Google Scholor - Pinheiro YA, Noah Y. (2019). Associations between female genital mutilation/cutting and HIV: a review of the evidence. Afr J AIDS Res. 18(3):181-191.
Publisher | Google Scholor - Mirastschijski U, Jiang D, Rinkevich Y. (2022). Genital wound repair and scarring. Med Sci. 10:23.
Publisher | Google Scholor - Eming SA, Martin P, Tomic-Canic M. (2014). Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med. 6(265):265sr6.
Publisher | Google Scholor - Kim HJ, Kim YH. (2024). Comprehensive insights into keloid pathogenesis and advanced therapeutic strategies. Int J Mol Sci. 25(16):8776.
Publisher | Google Scholor - Tan S, Khumalo N, Bayat A. (2019). Understanding keloid pathobiology from a quasi-neoplastic perspective: less of a scar and more of a chronic inflammatory disease with cancer-like tendencies. Front Immunol. 10:1810.
Publisher | Google Scholor - Lu YY, Tu HP, Wu CH, et al. (2021). Risk of cancer development in patients with keloids. Sci Rep. 11(1):9390.
Publisher | Google Scholor - Trace AP, Enos CW, Mantel A, et al. (2016). Keloids and hypertrophic scars: a spectrum of clinical challenges. Am J Clin Dermatol. 17(3):201-223.
Publisher | Google Scholor - Birge Ö, Akbaş M, Özbey EG, et al. (2016). Clitoral keloids after female genital mutilation/cutting. Turk J Obstet Gynecol. 13(3):154-157.
Publisher | Google Scholor - Morison L, Scherf C, Ekpo G, et al. (2001). The long-term reproductive health consequences of female genital cutting in rural Gambia: a community-based survey. Trop Med Int Health. 6(8):643-653.
Publisher | Google Scholor - Gauglitz GG, Korting HC, Pavicic T, et al. (2011). Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies. Mol Med. 17(1-2):113-125.
Publisher | Google Scholor - Coppa LM, Alam M, Longley BJ, et al. (1999). Eruptive paraneoplastic keloids. Cutis. 64:243-244.
Publisher | Google Scholor - He Y, Merin MR, Sharon VR, Maverakis E. (2011). Eruptive keloids associated with breast cancer: a paraneoplastic phenomenon? Acta Derm Venereol. 91(4):480-481.
Publisher | Google Scholor - Sakaguchi M, Fukumoto T, Fujishima F, et al. (2017). Bilateral breast keloids in an elderly woman associated with bilateral breast cancers and high concentration of serum tumor growth factor-β. J Dermatol. 44(11):1303-1308.
Publisher | Google Scholor - Hecken JM, Rezniczek GA, Tempfer CB. (2022). Innovative diagnostic and therapeutic interventions in cervical dysplasia: a systematic review of controlled trials. Cancers (Basel). 14:2670.
Publisher | Google Scholor - Włoszek E, Krupa K, Skrok E, et al. (2025). HPV and cervical cancer: biology, prevention, and treatment updates. Curr Oncol. 32(3):122.
Publisher | Google Scholor - Dasgupta S. (2022). A review on cervical dysplasia: etiology, risk factors, diagnostic biomarkers and possible nutritional association. Asian Pac J Cancer Care. 7(3):555-563.
Publisher | Google Scholor - Norenhag J, Du J, Olovsson M, et al. (2020). The vaginal microbiota, human papillomavirus and cervical dysplasia: a systematic review and network meta-analysis. BJOG. 127:171-180.
Publisher | Google Scholor - Ye J, Zheng L, He Y, et al. (2023). Human papillomavirus-associated cervical lesion: pathogenesis and therapeutic interventions. MedComm (2020). 4(5):e368.
Publisher | Google Scholor - Klein E, Helzner E, Shayowitz M, et al. (2018). Female genital mutilation: health consequences and complications – a short literature review. Obstet Gynecol Int. 7365715.
Publisher | Google Scholor - Martinez AA, Malinverno MU, Manin E, et al. (2021). A cross-sectional study on the prevalence of cervical dysplasia among women with female genital mutilation/cutting. J Low Genit Tract Dis. 25(3):210-215.
Publisher | Google Scholor - Altunkurek ŞZ, Yeşilyurt E, Hassan Mohamed S. (2024). Comparison of menstrual symptoms in university students with and without female genital mutilation/cutting. Int J Womens Health. 16:1451-1462.
Publisher | Google Scholor - Fink G, Abdulcadir J, Johnson-Agbakwu CE. (2023). Rates of cervical cancer screening and dysplasia among refugees in a health care safety net system. J Immigr Minor Health. 25(6):1315-1322.
Publisher | Google Scholor - Frick A, Azuaga A, Abdulcadir J. (2022). Cervical dysplasia among migrant women with female genital mutilation/cutting type III: a cross-sectional study. Int J Gynaecol Obstet. 157(3):557-563.
Publisher | Google Scholor - Jolidon V, De Prez V, Willems B, et al. (2020). Never and under cervical cancer screening in Switzerland and Belgium: trends and inequalities. BMC Public Health. 20(1):1517.
Publisher | Google Scholor - World Health Organization. (2016). Guidelines on the management of health complications from female genital mutilation. Geneva: WHO.
Publisher | Google Scholor - Vallejo-Ruiz V, Gutiérrez-Xicoténcatl L, Medina-Contreras O, et al. (2024). Molecular aspects of cervical cancer: a pathogenesis update. Front Oncol. 14:1356581.
Publisher | Google Scholor - Walboomers JMM, Jacobs MV, Manos MM, et al. (1999). Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 189:12-19.
Publisher | Google Scholor - Ogah J, Kolawole O, Awelimobor D. (2019). High-risk human papillomavirus common among a cohort of women with female genital mutilation. Afr Health Sci. 19(4):2985-2992.
Publisher | Google Scholor - Thomas JO, Herrero R, Omigbodun AA, et al. (2004). Prevalence of papillomavirus infection in women in Ibadan, Nigeria: a population-based study. Br J Cancer. 90:638-645.
Publisher | Google Scholor - Sharifah N, Seeni A, Nurismah MI, et al. (2009). Prevalence of human papillomavirus in abnormal cervical smears in Malaysian patients. Asian Pac J Cancer Prev. 10:303-306.
Publisher | Google Scholor - Bayo S, Bosch FX, de Sanjose S, et al. (2002). Risk factors of invasive cervical cancer in Mali. Int J Epidemiol. 31:202-209.
Publisher | Google Scholor - Wall S, Scherf C, Morison L, et al. (2005). Cervical human papillomavirus infection and squamous intraepithelial lesions in rural Gambia, West Africa: viral sequence analysis and epidemiology. Br J Cancer. 93(10):1068-1076.
Publisher | Google Scholor - Garba B, Sh Nur MA, Adawe M, et al. (2024) uman papillomavirus DNA detection in cervical samples from women of reproductive age in Mogadishu, Somalia. J Infect Dev Ctries. 18(11):1746-1755.
Publisher | Google Scholor - Petrelli A, Di Napoli A, Giorgi Rossi P, et al. Prevalence of primary HPV in Djibouti: feasibility of screening for early diagnosis of squamous intraepithelial lesions. J Low Genit Tract Dis. 20(4):321-326.
Publisher | Google Scholor - Tounkara FK, Téguété I, Guédou FA, et al. (2020). Human papillomavirus genotype distribution and factors associated among female sex workers in West Africa. PLoS One. 15(11):e0242711.
Publisher | Google Scholor - el-All HS, Refaat A, Dandash K. (2007). Prevalence of cervical neoplastic lesions and human papilloma virus infection in Egypt: National Cervical Cancer Screening Project. Infect Agent Cancer. 2:12.
Publisher | Google Scholor - Youssef MA, Abdelsalam L, Harfoush RA, et al. (2016). Prevalence of human papilloma virus (HPV) and its genotypes in cervical specimens of Egyptian women by linear array HPV genotyping test. Infect Agent Cancer. 11:6.
Publisher | Google Scholor - Abate E, Aseffa A, El-Tayeb M, et al. (2013). Genotyping of human papillomavirus in paraffin-embedded cervical tissue samples from women in Ethiopia and the Sudan. J Med Virol. 85(2):282-287.
Publisher | Google Scholor - Mboumba Bouassa RS, Nodjikouambaye ZA, Sadjoli D, Adawaye C, Péré H, et al. (2019). High prevalence of cervical high-risk human papillomavirus infection mostly covered by Gardasil-9 prophylactic vaccine in adult women living in N’Djamena, Chad. PLoS One. 14(6).
Publisher | Google Scholor - De Vuyst H, Parisi MR, Karani A, et al. (2010). The prevalence of human papillomavirus infection in Mombasa, Kenya. Cancer Causes Control. 21:2309-2313.
Publisher | Google Scholor - de Sanjosé S, Diaz M, Castellsagué X, et al. (2007). Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis. Lancet Infect Dis. 7(7):453-459.
Publisher | Google Scholor - Batyra E, Coast E, Wilson B, et al. (2020). The socioeconomic dynamics of trends in female genital mutilation/cutting across Africa. BMJ Glob Health. 5(10):e003088.
Publisher | Google Scholor - Ayenew AA, Mol BW, Bradford B, et al. (2023). Prevalence of female genital mutilation and associated factors among daughters aged 0–14 years in sub-Saharan Africa: a multilevel analysis of recent demographic health surveys. Front Reprod Health. 5:1105666.
Publisher | Google Scholor - Luoga P, Paulo HA, Mbishi JV, et al. (2025). Prevalence and determinants of female genital mutilation: current insights from ten at-risk countries in sub-Saharan Africa. BMC Public Health. 25:1031.
Publisher | Google Scholor - Hurtado-Salgado E, Ortiz-Panozo E, Salmerón J, et al. (2023). Prevalence of cervical human papillomavirus in Mexico, 2010-2017: analysis of 2.7 million women. Cancer Causes Control. 34(2):123-132.
Publisher | Google Scholor - Bruni L, Diaz M, Castellsagué X, et al. (2010). Cervical human papillomavirus prevalence in five continents: meta-analysis of one million women with normal cytological findings. J Infect Dis. 202(12):1789-1799.
Publisher | Google Scholor - Ortensi LE, Menonna A. (2017). Migrating with special needs? Projections of flows of migrant women with female genital mutilation/cutting toward Europe 2016-2030. Eur J Popul. 33(4):559-583.
Publisher | Google Scholor - United Nations Population Fund. (2011). Project Embera-wera: an experience of culture change to eradicate female genital mutilation in Colombia - Latin America. New York: UNFPA.
Publisher | Google Scholor - World Bank. (2021). FGM in Latin America among the Embera people in Colombia, Panama, and Ecuador.
Publisher | Google Scholor - Allali M, El Fermi R, Errafii K, et al. (2025). HPV genotypes in Africa: comprehensive analysis of genetic diversity and evolutionary dynamics. Arch Virol. 170(6):116.
Publisher | Google Scholor - Campos-Romero A, Anderson KS, Longatto-Filho A, et al. (2019). The burden of 14 hr-HPV genotypes in women attending routine cervical cancer screening in 20 states of Mexico: a cross-sectional study. Sci Rep. 9(1):10094.
Publisher | Google Scholor - Nascimento MDDSB, Vidal FCB, Silva MACND, et al. (2018). Prevalence of human papillomavirus infection among women from quilombo communities in northeastern Brazil. BMC Women’s Health. 18(1):1.
Publisher | Google Scholor - Li K, Li Q, Song L, et al. (2019). The distribution and prevalence of human papillomavirus in women in mainland China. Cancer. 125(7):1030-1037.
Publisher | Google Scholor - Brotherton JM, Hawkes D, Sultana F, et al. (2019). Age-specific HPV prevalence among 116,052 women in Australia’s renewed cervical screening program: a new tool for monitoring vaccine impact. Vaccine. 37(3):412-416.
Publisher | Google Scholor - Bao YP, Li N, Smith JS, et al. (2008). Human papillomavirus type-distribution in the cervix of Chinese women: a meta-analysis. Int J STD AIDS. 19(2):106-111.
Publisher | Google Scholor - Al-Awadhi R, Chehadeh W, Kapila K. (2011). Prevalence of human papillomavirus among women with normal cervical cytology in Kuwait. J Med Virol. 83(3):453-460.
Publisher | Google Scholor - Shanaka KASN, Wilathgamuwa S, Gunawardene YINS, et al. (2018). Prevalence of human papilloma virus and their high-risk genotypes in Sri Lankan women. Virusdisease. 29(1):27-31.
Publisher | Google Scholor - Li Z, Liu F, Cheng S, et al. (2016). HPV infection among 28,457 Chinese women in Yunnan Province, southwest China. Sci Rep. 6:21039.
Publisher | Google Scholor - Kouba LJ, Muasher J. (1985). Female circumcision in Africa: an overview. Afr Stud Rev. 28:95-110.
Publisher | Google Scholor - Bruni L, Barrionuevo-Rosas L, Albero G, et al. (2023). Human papillomavirus and related diseases in Egypt. ICO Information Centre on HPV and Cancer.
Publisher | Google Scholor - Nayel MA, Shaker OG, Hosni AN, et al. (2016). Human papillomavirus (HPV) in Egyptian females: study by cytology, histopathology, colposcopy and molecular diagnosis of high-risk types. Malays J Pathol. 38(3):257-266.
Publisher | Google Scholor - Deutsche Welle. (2020). Female genital mutilation: 68,000 victims in Germany. DW.
Publisher | Google Scholor - Deleré Y, Remschmidt C, Leuschner J, et al. (2014). Human papillomavirus prevalence and probable first effects of vaccination in 20- to 25-year-old women in Germany: a population-based cross-sectional study via home-based self-sampling. BMC Infect Dis. 14:87.
Publisher | Google Scholor - Bruni L, Albero G, Serrano B, et al. (2023). Human papillomavirus and related diseases in Germany. ICO/IARC Information Centre on HPV and Cancer.
Publisher | Google Scholor - De Schrijver L, Van Baelen L, Van Eekert N, et al. (2020). Towards a better estimation of prevalence of female genital mutilation in the European Union: a situation analysis. Reprod Health. 17:105.
Publisher | Google Scholor - Bruni L, Albero G, Rowley J, et al. (2023). Global and regional estimates of genital human papillomavirus prevalence among men: a systematic review and meta-analysis. Lancet Glob Health. 11(9):e1345-1362.
Publisher | Google Scholor























