

Research Article
Determinants of The Announcement of The Diagnosis of Their Infection to Children and Adolescents Living with HIV/AIDS in A Care Centre in Yaounde
- Epée Ngoué Jeannette 1*
- Mekone Nkwele Isabelle 1
- Douanla Nguetsa Guylaine 1
- Tony Nengom Jocelyn 3
- Kago Tague Daniel 1
- Meguieze Claude-Audrey 1
- Sime Tchouamo Arielle 2
- Kamgaing Nelly 1
- Koki Ndombo Paul 3
1Faculty of Medicine and Biomedical Sciences, University of Yaoundé 1, Cameroon.
2Faculty of Medicine and Pharmaceutical Sciences, University of Dschang, Cameroon.
3Mother and Child Center, Chantal Biya Foundation, Cameroon.
*Corresponding Author: Epée Ngoué Jeannette, Faculty of Medicine and Biomedical Sciences, University of Yaoundé 1, Cameroon.
Citation: Jeannette EN, Isabelle MN, Guylaine DN, Jocelyn TN, Daniel KT, et al. (2026). Determinants of The Announcement of The Diagnosis of Their Infection to Children and Adolescents Living with HIV/AIDS in A Care Centre in Yaounde. Journal of Clinical Paediatrics and Child Health Care, BioRes Scientia Publishers. 3(1):1-11. DOI: 10.59657/2997-6111.brs.26.025
Copyright: © 2026 Epée Ngoué Jeannette, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 22, 2025 | Accepted: February 26, 2026 | Published: March 20, 2026
Abstract
Introduction: The disclosure of HIV infection diagnosis to children and adolescents is a major challenge in therapeutic education, follow-up, and patient survival. However, the disclosure rate remains low in low- and middle-income countries. The objective of this study was to identify the factors that determine the disclosure of HIV infection diagnosis to infected children and adolescents (C/AHIV).
Materials and Methods: We conducted a case-control study involving the parents/guardians of children and adolescents aged 6 to 19 years living with HIV, followed at the Approved Therapeutic Center of the mother and Child Foundation Chantal Biya. Cases and controls were matched based on parental characteristics. From June to July 2023, using a semi-structured questionnaire, we collected sociodemographic data on C/AHIV and their parents/guardians, therapeutic aspects, and information regarding the disclosure of diagnosis. These data were entered using CsPro version 7.7.3 and analyzed using R and RStudio software. Factors associated with the disclosure of diagnosis were investigated using the Chi-square test or Fisher's Exact test. The odds ratio (with a 95% confidence interval) was used to measure the strength of the association of these factors with the disclosure of diagnosis.
Results: We included 27 cases and 54 controls, totaling 81 parents/guardians, of whom 85.2% were female. The average age was 44.8 ± 12.2 years. The diagnosis of infection was disclosed to C/AHIV at an average age of 11.8 ± 1.9 years. Disclosure was significantly associated with the child's age (p<0.001), Protestant religion (p=0.005), primary education level (p<0.001), living with at least one biological parent (p=0.008), discovering HIV infection in the context of illness (p=0.005), and the duration of ART since initiation (p<0.001). The age of the parent/guardian (p=0.002) was correlated with the disclosure of diagnosis. Belonging to a support group (p=0.017), participation in therapeutic education sessions (p=0.004), knowledge of another child living with HIV in the community (p=0.015), and the presence of another person living with HIV at home (p=0.048) were also significantly associated with the disclosure of diagnosis.
Conclusion: The determinants of disclosing the diagnosis of HIV infection to C/AHIV are multiple. Understanding modifiable factors and working to improve them could increase the rate of diagnosis disclosure in our context.
Keywords: HIV/AIDS; child; adolescent; diagnosis disclosure
Introduction
HIV infection remains a major public health problem globally, responsible for millions of deaths. In 2022, 39 million people were living with HIV worldwide, nearly two-thirds of whom were in the African region. Children aged 0 to 14 years accounted for 1.5 million [1]. In Cameroon, in 2022, the National Committee for the Fight Against AIDS estimated the overall prevalence of HIV/AIDS at 2.4%, down from 3.1% in 2018 [2]. UNAIDS also reported that Cameroon remains one of the most affected countries in Sub-Saharan Africa, with children under 15 years representing 7.96% of people living with HIV [1]. According to the CAMPHIA report evaluating the impact of HIV in the population of Cameroon published in 2020, the prevalence of HIV among children aged 0 to 19 years was 2.8% [7]. In 2022, according to Spectrum estimates, there were 29,168 children under 15 years living with HIV and 16,719 adolescents aged 15 to 19 infected, although new HIV infections have seen a significant decrease of 32% among children from 2020 to 2022 [2].
With the adoption of systematic counseling and testing, the "Test and Treat" strategy, and the use of highly active antiretroviral therapy (HAART), the survival rate of children infected with HIV has significantly increased [1]. They are now reaching adolescence, a period of great vulnerability and self-assertion that can lead to interruptions in antiretroviral treatment and medical follow-up, difficulties in treatment adherence, mental health issues, therapeutic failures, and the risk of HIV transmission to uninfected sexual partners. These challenges are exacerbated by the late disclosure of their HIV status [3,4].
The disclosure of HIV/AIDS diagnosis in children is a major issue in therapeutic education and consequently in patient follow-up and survival [5]. Indeed, a literature review conducted in 2017 exploring the outcomes of diagnosis disclosure on various aspects of patient health revealed that it helps slow the progression of the disease and supports better treatment adherence. Conversely, no-disclosure was associated with a decline in CD4 counts and an increase in mortality cases [6]. However, studies conducted in Sub-Saharan Africa, where pediatric infections remain numerous, show low rates of diagnosis disclosure to infected children, although these values vary from country to country. A systematic review conducted in 2016 in low- and middle-income countries revealed that only 1.7% to 41% of children aged 5 to 17 years infected with HIV/AIDS had received partial or complete disclosure of their serostatus [7]. In light of this issue, we conducted this study with the aim of determining the factors associated with the disclosure of diagnosis to children and adolescents infected with HIV/AIDS in a pediatric hospital in Cameroon.
Materials and Methods
We conducted an observational case-control study at the Day Unit of the mother and Child Center of the Chantal Biya Foundation (CME/FCB), which is one of the approved treatment centers (CTA) in Yaoundé, Cameroon. The study period extended from July to August 2023.
The observation variable was whether a parent had previously initiated the process of disclosing the HIV/AIDS diagnosis. The exposure variables were diverse, ranging from sociodemographic characteristics of both parents and patients to treatment-related and social assistance factors.
Included as cases, after obtaining their informed consent, were the parents/guardians of children and adolescents aged 6 to 19 years living with HIV/AIDS who were followed at the center and had already initiated the process of disclosing the diagnosis to their children. The controls were the parents/guardians of children and adolescents living with HIV (C/AHIV) who had not yet done so.
We conducted a no-probabilistic, consecutive, and exhaustive sampling of parents/guardians meeting our inclusion criteria. The minimum sample size was calculated to be 16 cases and 32 controls using Schlesselman’s formula [8]. Controls were matched to cases by taking eligible parents who attended consultations within the following 24 hours after a case was included.
Upon arrival, both parents and their children were received at the reception service, where their care began. We then explained the purpose of the study, and after obtaining informed consent, we conducted interviews after their visit to the pharmacy. To avoid accidental disclosure for children and adolescents living with HIV (C/AHIV) who were not yet informed of their serostatus, we administered the questionnaire privately to the parent/guardian.
The pre-designed questionnaire for data collection consisted of three essential parts: data related to the patient (sociodemographic, medical, paramedical), data concerning the guardian (sociodemographic, serostatus, social assistance modalities), and data related to the diagnosis disclosure (level of disclosure, reasons for no-disclosure).
Qualitative factors associated with diagnosis disclosure were investigated using the Chi-square test or Fisher's Exact test, depending on whether the theoretical counts were greater than or equal to 5, or less than 5. The odds ratio (with a 95% confidence interval) was used to measure the strength of the association of these factors with diagnosis disclosure. A multivariate analysis using logistic regression, including factors significantly associated with disclosure, was performed to exclude the effect of confounding factors. The significance threshold was set at 5%.
Results
A total of 81 parents/guardians of children and adolescents living with HIV followed at the CME/FCB were enrolled, comprising 27 cases and 54 controls (Figure 1). Sixty-nine parents/guardians included in our study were female, accounting for 85.2% of the study population. The sex ratio was 0.17. Their mean age was 44.8 ± 12.2 years, with a median of 42 years and extremes of 23 and 76 years. Fifty-one parents/guardians (63.0%) had a positive serology (Table 1).
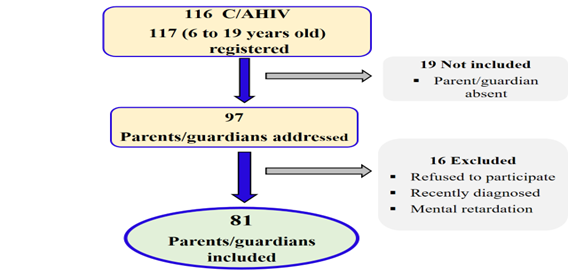
Figure 1: Participant flow diagram.
Table 1: Socio demographic characteristics of C/AHIV.
| Characteristics | Cases n=271 | Controls n=541 | Total n=811 |
| Age (years) | |||
| Mean ± SD | 15.6 ± 2.2 | 9.3 ± 2.5 | 11.5 ± 3.9 |
| Median [IQR] | 16.5 [13.0 - 17.0] | 9.0 [7.0 - 11.0] | 11.0 [8.0 - 15.0] |
| Range | 11.0 - 19.0 | 6.0 - 15.0 | 6.0 - 19.0 |
| Sex | |||
| Female | 18 (39.1) | 28 (60.9) | 46 (56.8) |
| Male | 10 (28.6) | 25 (71.4) | 35 (43.2) |
| Religion | |||
| Catholic | 11 (22.9) | 37 (77.1) | 48 (59.3) |
| Protestant | 9 (69.2) | 4 (30.8) | 13 (16.0) |
| Pentecostal | 5 (38.5) | 8 (61.5) | 13 (16.0) |
| Muslim | 1 (20.0) | 4 (80.0) | 5 (6.2) |
| Other | 1 (50.0) | 1 (50.0) | 2 (2.5) |
| Region of origin | |||
| Fang-Beti | 16 (2.6) | 40 (76.9) | 56 (69.1) |
| Grassfields | 6 (37.5) | 10 (62.5) | 16 (19.8) |
| Sudano-sahelian | 2 (66.7) | 1 (33.3) | 6 (7.4) |
| Sawa | 3 (50.0) | 3 (50.0) | 3 (3.7) |
| Level of education | |||
| Primary | 22 (68.7) | 10 (31.3) | 48 (59.3) |
| Secondary | 0 (0.0) | 1 (100.0) | 32 (39.5) |
| Not educated | 5 (10.4) | 43 (89.6) | 1 (1.2) |
| Residence | |||
| Family member | 13 (52.0) | 12 (48.0) | 25 (30.9) |
| Biological parents | 14 (25.0) | 42 (75.0) | 56 (69.1) |
| Orphan | |||
| No | 13 (26.5) | 36 (73.5) | 49 (60.5) |
| Yes | 14 (43.8) | 18 (56.3) | 32 (39.5) |
| If yes, specify | |||
| Both parents deceased | 2 (33.3) | 4 (66.7) | 6 (18.8) |
| Mother deceased | 8 (57.1) | 6 (42.9) | 13 (40.6) |
| Father deceased | 4 (33.3) | 8 (66.7) | 13 (40.6) |
| 1n (%) | |||
The mean age of the children and adolescents was 11.5 ± 3.9 years, with a median of 11 years and extremes of 6 and 19 years. The most represented age groups were 6 to 8 years and 15 to 19 years. Females predominated, with a frequency of 56.8% (n=46). More than half of the children and adolescents living with HIV (59.3%, n=48) were of Catholic faith. Most (69.1%) lived with at least one biological parent (n=56), among whom 32 (39.5%) were orphans (Table 2).
Table 2: Socio demographic characteristics of parent/guardian.
| Characteristics | Number n=81 | Percentages (%) |
| Age of parent/guardian (in years) | ||
| Mean ± SD | 44.8 ± 12.2 | |
| Median [IQR] | 42.0 [37.0 - 51.0] | |
| Interval | 23.0 - 76.0 | |
| Gender of parent/guardian | ||
| Female | 69 | 85,2 |
| Male | 12 | 14,8 |
| Level of education parent/guardian | ||
| Primary | 20 | 24,7 |
| Secondary | 54 | 66,7 |
| Superior | 7 | 8,6 |
| Profession parent/guardian | ||
| Civil servant | 23 | 28,4 |
| Liberal | 38 | 46,9 |
| Unemployed | 15 | 18,5 |
| Retired | 5 | 6,2 |
| Marital status | ||
| Single | 15 | 18,5 |
| Cohabitation | 24 | 29,6 |
| Married | 21 | 25,9 |
| Widow | 18 | 22,2 |
| Divorced | 3 | 3,7 |
| Serological status of parent/guardian | ||
| Positive | 52 | 64,2 |
| Negative | 29 | 35,8 |
The HIV infection was diagnosed on average 2.9 ± 2.7 years ago, with a median of 2 years. The mode of discovery was primarily in the context of illness, accounting for 58.0% of cases, followed by index cases in 23.5%, during PMTCT follow-up in 17.3%, and through systematic testing in 1.2% of cases. In 90% of cases, the transmission was vertical, meaning from mother to child. Only 2 children were infected through horizontal transmission: one following a blood transfusion and the other through contaminated sharp objects. The median duration of ARV treatment was 87.5 months (7.29 years). Most children and adolescents living with HIV were on first-line treatment (92.6%), and 82.7% had an undetectable viral load at their last check. Only 46.9% were regularly taking their Cotrimoxazole prophylaxis.
The residence in urban areas concerned 63 parents/guardians (77.8%). Forty-eight biological mothers (59.3%) were recorded as parents/guardians of children and adolescents living with HIV (C/AHIV). These children lived in households with an average of 5.9 ± 2.5 inhabitants.
In terms of social assistance, 30 parents/guardians (37.0%) received a subsidy for the care and needs of the child, granted by an NGO in 90.0% of cases. Only 12 parents/guardians (14.8%) belonged to a support group, 19 (23.5%) participated in therapeutic education sessions or support groups with or without their children, and 14 (17.3%) knew another child infected with HIV in the community (Table 4).
Data Related to Diagnosis Disclosure
In the case group, the diagnosis was disclosed between the ages of 9 and 15 years. The mean age at disclosure was 11.8 ± 1.9 years, with a median of 12 years. In this population, the disclosure was conducted by a healthcare professional for more than half of the patients, specifically 55.6% (n=15). Individual disclosure was the preferred type, practiced for 85.2% (n=23) of these patients (Table 3).
Determinants of Disclosure (Table IV).
Table 3: Distribution according to the circumstances of the diagnosis.
| Characteristics | Number n = 27 | Percentages (%) |
| Stage of the disease at the time of diagnosis | ||
| Stage I | 24 | 88.9 |
| Stage II | 2 | 7.4 |
| Stage III | 1 | 3.7 |
| Person who made the announcement | ||
| Parent/Guardian | 9 | 33.3 |
| Healthcare staff | 15 | 55.6 |
| Other | 3 | 11.1 |
| Type of announcement | ||
| Collective | 4 | 14.8 |
| Individual | 23 | 85.2 |
Table 4: Factors associated with the announcement.
| Characteristics | Announcement of diagnosis | OR2 | 95% CI2 | p-value | |
| Yes n = 271 | No n = 541 | ||||
| Sex | |||||
| Female | 17 (37.0%) | 29 (63.0%) | Ref. | Ref. | |
| Male | 10 (28.6%) | 25 (71.4%) | 0.62 | 0.24, 1.58 | 0.324 |
| Age (years) | |||||
| Mean ± SD | 15.6 ± 2.2 | 9.3 ± 2.5 | less than 0.001 | ||
| Age groups (years) | |||||
| [15,19] | 19 (86.4%) | 3 (13.6%) | Ref. | Ref. | |
| [6,9[ | 0 (0.0%) | 22 (100.0%) | NA | NA | 0.992 |
| [9,12[ | 1 (4.8%) | 20 (95.2%) | 0.01 | 0.0001, 0.04 | less than 0.001 |
| [12,15[ | 7 (43.8%) | 9 (56.3%) | 0.08 | 0.01, 0.39 | 0.004 |
| Religion | |||||
| Catholic | 11 (22.9%) | 37 (77.1%) | Ref. | Ref. | |
| Protestant | 9 (69.2%) | 4 (30.8%) | 6.75 | 1.85, 28.8 | 0.005 |
| Pentecost | 5 (38.5%) | 8 (61.5%) | 1.88 | 0.49, 6.80 | 0.341 |
| Muslim | 1 (20.0%) | 4 (80.0%) | 0.75 | 0.04, 5.72 | 0.805 |
| Other | 1 (50.0%) | 1 (50.0%) | 3.00 | 0.11, 79.9 | 0.450 |
| Level of study | |||||
| Secondary | 22 (68.7%) | 10 (31.3%) | Ref. | Ref. | |
| No study | 0 (0.0%) | 1 (100.0%) | NA | NA | 0.991 |
| Primary | 5 (10.4%) | 43 (89.6%) | 0.05 | 0.01, 0.14 | less than 0.001 |
| Residence | |||||
| Family member | 13 (52.0%) | 12 (48.0%) | Ref. | Ref. | |
| Biological parents | 14 (25.0%) | 42 (75.0%) | 0.26 | 0.09, 0.70 | 0.008 |
| Orphelin | |||||
| No | 13 (26.5%) | 36 (73.5%) | Ref. | Ref. | |
| Yes | 14 (43.8%) | 18 (56.3%) | 1.94 | 0.77, 5.00 | 0.163 |
| Age at diagnosis (in years) | |||||
| Mean ± SD | 3.1 ± 3.2 | 2.7 ± 2.5 | 0.486 | ||
| Median [IQR] | 2.0 [1.0 - 4.3] | 2.0[1.0-4.0] | |||
| Range | 0.0 - 11.0 | 0.0 - 10.0 | |||
| Age range at diagnosis (years) | |||||
| [0,3[ | 18 (34.6%) | 34 (65.4%) | Ref | Ref | |
| [3,6[ | 3 (21.4%) | 11 (78.6%) | 0.47 | 0.10, 1.75 | 0.294 |
| [6,9[ | 2 (22.2%) | 7 (77.8%) | 0.50 | 0.07, 2.31 | 0.411 |
| [9,11] | 4 (66.7%) | 2 (33.3%) | 3.47 | 0.62, 26.8 | 0.172 |
| Discovery mode | |||||
| Screening following an index case | 10 (52.6%) | 9 (47.4%) | Ref. | Ref. | |
| Systematic screening | 0 (0.0%) | 1 (100.0%) | NA | NA | 0.991 |
| Disease stage | 10 (21.3%) | 37 (78.7%) | 0.20 | 0.06, 0.61 | 0.005 |
| Antenatal Exposure follow-up | 7 (50.0%) | 7 (50.0%) | 0.73 | 0.18, 2.93 | 0.653 |
| Stage of disease at diagnosis | |||||
| Stage I | 17 (47.2%) | 19 (52.8%) | Ref. | Ref. | |
| Stage II | 5 (35.7%) | 9 (64.3%) | 0.56 | 0.15, 1.94 | 0.366 |
| Stage III | 2 (10.5%) | 17 (89.5%) | 0.12 | 0.02, 0.49 | 0.009 |
| Stage IV | 3 (25.0%) | 9 (75.0%) | 0.33 | 0.07, 1.33 | 0.140 |
| Mode de transmission | |||||
| Vertical | 22 (30.1%) | 51 (69.9%) | Ref. | Ref. | |
| Horizontal | 1 (50.0%) | 1 (50.0%) | 2.17 | 0.08, 56.6 | 0.589 |
| Inconnu | 4 (66.7%) | 2 (33.3%) | 4.35 | 0.79, 33.0 | 0.103 |
| ARVT duration (months) | |||||
| Mean ± SD | 145.4 ± 56.2 | 79.6 ± 31.0 | |||
| Median [IQR] | 164.0 [105.5 - 189.3] | 80.5 [65.5 - 98.6] | less than 0.001 | ||
| ARVT duration | |||||
| less than 60 months | 2 (18.2%) | 9 (81.8%) | Ref. | Ref. | |
| [60 - 120[ | 6 (12.8%) | 41 (87.2%) | 0.39 | 0.08, 2.14 | 0.243 |
| [120 - 180[ | 8 (66.7%) | 4 (33.3%) | 5.33 | 0.96, 36.9 | 0.067 |
| >= 180 | 11 (100.0%) | 0 (0.0%) | NA | NA | 0.992 |
| Current ARV treatment | |||||
| 1st line | 24 (32.0%) | 51 (68.0%) | Ref. | Ref. | |
| 2nd line | 3 (50.0%) | 3 (50.0%) | 2.00 | 0.35, 11.5 | 0.416 |
| Last viral load | |||||
| Detected | 5 (35.7%) | 9 (64.3%) | Ref. | Ref. | |
| Undetectable | 22 (32.8%) | 45 (67.2%) | 0.65 | 0.20, 2.20 | 0.475 |
| Age of parent/guardian | |||||
| Mean ± SD | 50.8 ± 11.3 | 41.6 ± 11.5 | 0.002 | ||
| Parent/guardian age range | |||||
| [65,76] | 2 (33.3%) | 4 (66.7%) | Ref. | Ref. | |
| [23,25[ | 0 (0.0%) | 1 (100.0%) | NA | NA | 0.991 |
| [25,35[ | 2 (12.5%) | 14 (87.5%) | 0.14 | 0.01, 1.20 | 0.080 |
| [35,45[ | 5 (17.9%) | 23 (82.1%) | 0.22 | 0.03, 1.46 | 0.110 |
| [45,55[ | 11 (61.1%) | 7 (38.9%) | 1.57 | 0.23, 10.8 | 0.634 |
| Level of study parent/guardian | |||||
| Primary | 7 (35.0%) | 13 (65.5%) | Ref. | Ref. | |
| Secondary | 17 (31.5%) | 37 (68.5%) | 0.69 | 0.24, 2.04 | 0.493 |
| Superior | 3 (42.9%) | 4 (57.1%) | 1.13 | 0.18, 6.52 | 0.895 |
| Profession parent/tguardian | |||||
| Civil servant | 11 (40.9%) | 13 (50.1%) | Ref. | Ref. | |
| Libéral | 12 (31.6%) | 26 (68.4%) | 0.55 | 0.19, 1.64 | 0.285 |
| Unemployed | 3 (60.0%) | 2 (40.0%) | 1.80 | 0.25, 15.8 | 0.560 |
| Retired | 3 (18.7%) | 13 (81.3%) | 0.30 | 0.06, 1.27 | 0.120 |
| Matrimonial status | |||||
| Single | 3 (20.0%) | 12 (80.0%) | Ref. | Ref. | |
| Cohabitation | 5 (20.8%) | 19 (79.2%) | 0.72 | 0.16, 3.46 | 0.675 |
| Married | 2 (66.7%) | 1 (33.3%) | 5.50 | 0.42, 140 | 0.209 |
| Widow | 11 (52.4%) | 10 (47.6%) | 3.03 | 0.76, 13.9 | 0.129 |
| Divorced | 6 (33.3%) | 12 (66.7%) | 1.38 | 0.31, 6.64 | 0.679 |
| Statut sérologique parent/guardian | |||||
| Negative | 13 (44.8%) | 16 (55.2%) | Ref. | Ref. | |
| Positive | 14 (27.5%) | 37 (72.5%) | 0.41 | 0.15, 1.05 | 0.063 |
| Inconnu | 0 (0.0%) | 1 (100.0%) | NA | NA | 0.992 |
| Tutor-patient relationship | |||||
| Father | 4 (33.3%) | 8 (66.7%) | Ref. | Ref. | |
| Grand-parent | 5 (41.7%) | 7 (58.3%) | 1.00 | 0.19, 5.19 | >0.999 |
| Mother | 12 (25.0%) | 36 (75.0%) | 0.47 | 0.12, 1.83 | 0.258 |
| Uncle | 3 (50.0%) | 3 (50.0%) | 1.40 | 0.19, 10.7 | 0.738 |
| Other | 3 (100.0%) | 0 (0.0%) | NA | NA | 0.990 |
| Another HIV seropositive in the | |||||
| No | 12 (46.2%) | 14 (53.8%) | Ref. | Ref. | |
| Yes | 15 (27.3%) | 40 (72.7%) | 0.38 | 0.14, 0.99 | 0.048 |
| Existence of a subsidy | |||||
| No | 19 (37.2%) | 32 (62.8%) | Ref | Ref | |
| Yes | 8 (26.7%) | 22 (73.3%) | 0.56 | 0.20, 1.48 | 0.254 |
| Membership of a support group | |||||
| No | 19 (27.5%) | 50 (72.5%) | Ref. | Ref. | |
| Yes | 8 (66.7%) | 4 (33.3%) | 4.90 | 1.38, 20.1 | 0.017 |
| Attendance education meetings | |||||
| No | 15 (24.2%) | 47 (75.8%) | Ref. | Ref. | |
| Yes | 12 (63.2%) | 7 (36.8%) | 4.93 | 1.69, 15.4 | 0.004 |
| Knowledge of other infected children in the community | |||||
| No | 18 (26.9%) | 49 (73.1%) | Ref. | Ref. | |
| Yes | 9 (64.3%) | 5 (35.7%) | 4.55 | 1.39, 16.5 | 0.015 |
| 1n (%) 2OR = Odds Ratio, CI = Confidence Interval ARVT: antiretroviral treatment HIV: Human Immunodeficiency Virus | |||||
Among the sociodemographic characteristics of C/AHIV, we found a statistically significant association between diagnosis disclosure and the child's age (p less than 0.001), particularly in the age groups of 9 to 11 years (p less than 0.001) and 12 to 14 years (p=0.004). Protestant religion (p=0.005), primary education level (p less than 0.001), and living with at least one biological parent (p=0.008) were also associated with diagnosis disclosure.
The duration of antiretroviral treatment since initiation (p less than 0.001) was correlated with diagnosis disclosure; however, no specific interval was identified. Regarding the sociodemographic characteristics of the parent/guardian, only age (p=0.002) was recognized as a significantly associated factor with diagnosis disclosure. In terms of social assistance, diagnosis disclosure was significantly associated with the presence of another person infected with HIV at home (p=0.048), the child's or parent's membership in a support group (p=0.017), participation in therapeutic education sessions (p=0.004), and knowledge of another child infected in the community (p=0.015).
Discussion
Our objective was to identify the factors that determine the disclosure of HIV infection diagnosis to children and adolescents living with HIV followed at the mother and Child Center of the Chantal Biya Foundation. In this case-control study, we enrolled 81 parents/guardians of C/AHIV (27 cases and 54 controls) from whom we collected information related to the child, their parent/guardian, and the disclosure of the diagnosis. It emerged that the disclosure of their infection diagnosis to C/AHIV is primarily determined by factors related to the child and their treatment, as well as those related to their parent/guardian and the modalities of social assistance provided to the child.
The few limitations recognized in this study-such as loss to follow-up, incomplete patient records, and certainty bias in some statements-did not compromise the quality of our observations and their final relevance. The most represented age groups were 6 to 8 years and 15 to 19 years. A different distribution was found by Gyamfi et al. [9], who reported a predominance of children aged 6 to 10 years and 11 to 15 years, with respective frequencies of 36.8% and 28.9%. We found a statistically significant association between the child's age and the disclosure of the diagnosis (p less than 0.001), particularly with the age groups of 9 to 12 years (p less than 0.001) and 12 to 15 years (p = 0.004). These ages correspond to the beginning of the child's awakening, characterized by significant questioning, and to adolescence, which represents a period of substantial changes, personality development, and a desire for autonomy [10]. These physiological elements create a stressful environment for the parent/guardian facing a child or adolescent who wants to know more about the reason for their daily medication and the endless hospital appointments. This stress is likely exacerbated if there are other children in the household who are not subjected to the same constraints. The influence of age on diagnosis disclosure has been reported in the literature by several authors [1,7,11,12-15]. Although the age groups are not always specified, an age over 10 years has often been linked to diagnosis disclosure.
Religion was identified in our study as a factor capable of influencing diagnosis disclosure, unlike the study by Biadgilign et al. [15], where the association between religion and disclosure was not found. In their study, religions were divided into two groups: Orthodox and others. In contrast, we analyzed them in more detail, allowing us to identify a statistically significant association between Protestant religion and diagnosis disclosure (p = 0.005).
Living with at least one biological parent favored disclosure (p = 0.008), but this was not the case for orphan status, which differed from Chanie et al. [13], who found an association between disclosure and the mother or guardian being widowed. Other authors have found a significant association with the absence or death of the father or the main guardian [7,16]. The influence of living with a biological parent on disclosure arises from the type of relationship that generally exists between the child and their biological parent; the often close and significant emotional bond prompts such a parent to care about the sick child's demands and pay attention to their needs, whether formally expressed or not. The parent seems better positioned to identify the timing and necessity of disclosing the diagnosis to the child.
Regarding the sociodemographic data of the parent/guardian, only the age of the parent/guardian was recognized as a significantly associated factor with diagnosis disclosure (p = 0.002). A similar result was found in Nigeria, where a parent/guardian age of 40 years or older favored disclosure [3]. The education level of the parent/guardian had no influence on diagnosis disclosure. However, in the literature, African studies have demonstrated a significant association between disclosure and a low education level of the parent/guardian [7], particularly with primary education [14].
Concerning the circumstances of HIV infection discovery, more than half of the sample (64.2%) was diagnosed between the ages of 0 and 3 years, with a mean age of 2.9 ± 2.7 years. This relatively early diagnosis age is linked to the predominance of vertical transmission of HIV (90.1%). However, it reflects a diagnostic delay that calls into question the effectiveness of PMTCT follow-up, especially regarding the turnaround time for early detection test results and the retention of exposed children in the continuum of care.
The discovery of the infection in a context of illness, particularly those classified as stage 3, was significantly associated with diagnosis disclosure. These results suggest that in the face of a serious situation during the illness, parents/guardians are more likely to inform the child or adolescent of their serostatus, aiming to encourage self-involvement in managing the disease and/or better adherence. We did not find any studies addressing this issue among those reviewed.
The presence of another person living with HIV at home was associated with diagnosis disclosure in our study (p = 0.048). This association could be explained by the fact that when the child or adolescent begins to question their individuality and future with the infection, or presents behavioural or emotional disturbances related to identity formation during puberty, identifying with someone close who shares the same situation might be comforting. Thus, disclosing a child's serologic status seems simpler when they are not the only one at home taking daily medication. Furthermore, when the person the child identifies with shows no physical signs of their infection and occupies an enviable position in the family or society, the C/AHIV can better manage the emotions surrounding the disclosure of their diagnosis and will be encouraged to adhere to treatment.
Among the therapeutic modalities examined, the mean duration of ARV treatment since initiation was 102.3 ± 51.8 months, and 92.6% of C/AHIV were on first-line ARV. An author in Uganda found an association between initiating ART and diagnosis disclosure [12]. The systematic review conducted by Britto et al. [7] in 2018 confirmed this result, specifying that a longer duration on ART influenced the conduct of diagnosis disclosure to C/AHIV. Indeed, with the advent of the "Test and Treat" strategy, children are started on treatment as soon as the infection is diagnosed and therefore spend many years on medication. This continuous exposure to medication will prompt questioning, creating an environment conducive to disclosing their diagnosis to the child. This explains the significant association between disclosure and duration of ARV treatment found in our sample.
The mean age at diagnosis disclosure in our study population was 11.8 ± 1.9 years, identical to that found in Nigeria in 2020 [16]. Other authors have reported a mean age lower than ours, ranging from 8.7 to 10.6 years [11,17]. These results align with WHO recommendations [18] regarding the age for complete diagnosis disclosure, although disclosure rates remain low in our populations. This suggests that when disclosure occurs, it is done in accordance with recommendations, but it is not done often enough even when children and adolescents are eligible. Indeed, in our series, parents/guardians who had not yet started or completed the disclosure process indicated they would prefer complete disclosure at a mean age of 13.4 ± 2.2 years, with extremes of 10 and 19 years. The desired age is quite late compared to the age recommended by WHO and other NGOs involved in paediatric HIV care [10,18], which is 12 years. This information further underscores the glaring lack of knowledge among parents/guardians regarding when and how to disclose to their children [9].
Several parents/guardians in our study population, specifically 68.5%, wanted to disclose the HIV infection diagnosis to their children themselves. This aligns with findings from studies conducted in Zimbabwe and Nigeria, which reported that 76.0% and 79.4% of disclosures were made by parents/guardians, respectively [19,20]. These parents/guardians generally tend to delay the disclosure, prompting healthcare personnel to do so in order to address urgent situations, such as poor treatment adherence or behavioural issues arising in the child or adolescent living with HIV. Thus, in our study, the disclosure was primarily conducted by healthcare personnel. This result is similar to that of Ethiopian authors in 2022, who found that 69.7% of disclosures were made by healthcare professionals [13]. A better understanding of the disclosure process would certainly help parents/guardians manage it better and disclose the HIV infection diagnosis to their children at their convenience, although healthcare personnel play a crucial role in assisting them in preparing the child for the disclosure. According to Abebe and Teferra [21] in Ethiopia, 86% of parents/guardians reported needing help from healthcare professionals to disclose the diagnosis. This information highlights the importance of both medical and social assistance for C/AHIV and their parents/guardians [22].
Thirty parents/guardians, or 37.0%, received a subsidy for the care and needs of the child, with 90.0% of these subsidies granted by an NGO. Chanie et al. [13] in Ethiopia in 2022 identified a correlation between diagnosis disclosure and support from an NGO. Indeed, the assistance provided by NGOs is not solely financial; it also encompasses other aspects such as the child's healthcare, their well-being, their perception of the illness, their education, and their social integration. Relay agents between NGOs and families provide moral support and advice that can encourage parents/guardians to proceed with the diagnosis disclosure when their children are eligible. The association between NGO support and diagnosis disclosure was not demonstrated in this study. This difference may be explained by the low proportion of parents/guardians (37.0%) who received a subsidy and reported that this assistance was not consistent over time.
Our analyses demonstrated that membership in a support group, as well as participation in therapeutic education sessions or support groups, were significantly associated with the disclosure of their children's HIV infection diagnosis. A similar result was found in a study conducted in Uganda in 2014, which also identified an association between disclosure and membership in a support group [12]. In the present study, low participation rates may have contributed to the low rate of diagnosis disclosure in our populations. Questions posed to healthcare personnel at the CME/FCB's CTA revealed that invitations to therapeutic education sessions were only sent to parents/guardians of C/AHIV who presented specific problems, such as poor treatment adherence, high viral load, or other therapeutic failures, behavioral issues, or aggression towards parents or guardians.
Knowledge of another child or adolescent infected with HIV in the community was significantly associated with diagnosis disclosure. In fact, community-infected adolescents sometimes play the role of community advisors or peer educators, providing valuable support due to their shared experience of the illness and treatments.
Conclusion
This study emphasizes that the disclosure of their HIV infection diagnosis to children and adolescents living with HIV followed at the CME/FCB occurred at a mean age of 11.8 ± 1.9 years. This disclosure was individual and preferentially conducted by healthcare personnel. The identified determinants of diagnosis disclosure were mainly: the age of the child or adolescent between 9 and 15 years, Protestant religion, primary education level, and living with at least one biological parent. The discovery of HIV infection in the context of illness, particularly a condition classified as stage 3, was significantly associated with diagnosis disclosure, as was the duration of ARV treatment. The age of the parent/guardian was the only characteristic correlated with diagnosis disclosure. Social factors were identified as determinants of diagnosis disclosure, including membership in a support group, participation in therapeutic education sessions or support groups, and knowledge of another child infected with HIV in the community.
Conflicts of Interest
None.
References
- Global HIV & AIDS statistics - Fact sheet. UNAIDS 2022.
Publisher | Google Scholor - Rapport annuel 2022 des activités de lutte contre le VIH. Comité National de Lutte contre le SIDA; CNLS Yaoundé, 2023.
Publisher | Google Scholor - Danjuma JS, Sambo MN, Umar AA, Olorukooba A, Oyefabi AM, et al. (2020). Predictors of pediatric HIV disclosure among caregivers of HIV positive children attending special treatment clinic in dalhatu araf specialist hospital, Lafia, Nigeria. Niger J Clin Pract., 23(6):857-863.
Publisher | Google Scholor - Dahourou D. (2019). Annoce à l’enfant et à l’adolescent de son statut VIH en Afrique francophone centrale et de l’Ouest. Bull Soc Pathol Exot., 112(1):114-118.
Publisher | Google Scholor - Peltier, A. (2007). Annoce du diagnostic d’infection par le VIH/Sida chez l’enfant : un enjeu majeur de l’éducation thérapeutique. Proposition d’une méthode d’annoce et d’outils didactiques utilisés depuis 1999 dans de nombreux pays. In : Développement et Santé., 187.
Publisher | Google Scholor - Odiachi A. (2017). The Impact of Disclosure on Health and Related Outcomes in Human Immunodeficiency Virus-Infected Children: A Literature Review. Front Public Health., 5:231.
Publisher | Google Scholor - Britto C, Mehta K, Thomas R, Shet A. (2016). Prevalence and Correlates of HIV Disclosure Among Children and Adolescents in Low- and Middle-Income Countries: A Systematic Review. J Dev Behav Pediatr., 37(6):496 505.
Publisher | Google Scholor - Fleiss JL, Bruce L. (1988). Sample size determination in with matched pairs. J clin epidemiol., 41(8):727-730.
Publisher | Google Scholor - Gyamfi E, Okyere P, Appiah-Brempong E, Adjei RO, Mensah KA. Benefits of Disclosure of HIV Status to Infected Children and Adolescents: Perceptions of Caregivers and Health Care Providers. Journal of the Association of Nurses in AIDS Care. 2015;26(6):770-780.
Publisher | Google Scholor - Masson D. (2010). Grandir : Guide sur l’annoce du VIH à l’enfant et à l’adolescent. Initiative Développement et Sidaction; (Grandir), Ed.
Publisher | Google Scholor - Brown BJ, Oladokun RE, Osinusi K, Ochigbo S, Adewole IF, et al . (2011). Disclosure of HIV status to infected children in a Nigerian HIV Care Programme. AIDS Care., 23(9):1053-1058.
Publisher | Google Scholor - Namasopo-Oleja S, Bagenda D, Ekirapa-Kiracho E. (2015). Factors affecting disclosure of serostatus to children attending Jinja Hospital Paediatric HIV clinic, Uganda. Afr H Sci., 15(2):344.
Publisher | Google Scholor - Chanie MG, Abebe A, Muche A, Worku N. (2022). HIV Positivity Disclosure Among Children Living with HIV/AIDS and Currently on HAART in Dessie, Northeast Ethiopia. HIV AIDS (Auckl)., 14:461-472.
Publisher | Google Scholor - Lemma T, Silesh M, Taye BT, Desta K, Kitaw TM, (2022). HIV Serostatus Disclosure and Its Predictors Among Children Living with HIV in Ethiopia: A Systematic Review and Meta-Analysis. Front Public Health., 10:859469
Publisher | Google Scholor - Biadgilign S, Deribew A, Amberbir A, Escudero HR, Deribe K. (2011). Factors Associated with HIV/AIDS Diagnostic Disclosure to HIV Infected Children Receiving HAART: A Multi-Center Study in Addis Ababa, Ethiopia. PLoS ONE., 6(3):e17572.
Publisher | Google Scholor - Mukhtar-Yola M, Kuczawski M, Oniyangi O. (2020). Should children know their HIV status? Prevalence, caregiver’s perspectives and barriers to disclosure at the National Hospital Abuja, Nigeria. Niger J Clin Pract., 23(10):1419-1425.
Publisher | Google Scholor - Hayfron-Benjamin A, Obiri-Yeboah D, Ayisi-Addo S, Siakwa PM, Mupepi S. (2018). HIV diagnosis disclosure to infected children and adolescents; challenges of family caregivers in the Central Region of Ghana. BMC Pediatr., 18(1):365.
Publisher | Google Scholor - (2011). Guideline on HIV disclosure counselling for children up to 12 years of age. World Health Organization(éd), Geneva., 18.
Publisher | Google Scholor - Finnegan A, Langhaug L, Schenk K, Puffer ES, Rusakaniko S, et al. (2019). The prevalence and process of pediatric HIV disclosure: A population-based prospective cohort study in Zimbabwe. PLoS ONE., 14(5): e0215659.
Publisher | Google Scholor - Odiachi A, Abegunde D. (2016). Prevalence and predictors of pediatric disclosure among HIV-infected Nigerian children on treatment. AIDS Care., 28(8):1046-1051.
Publisher | Google Scholor - Abebe W, Teferra S. (2012). Disclosure of diagnosis by parents and caregivers to children infected with HIV: prevalence associated factors and perceived barriers in Addis Ababa, Ethiopia. AIDS Care., 24(9):1097-1102.
Publisher | Google Scholor - Njom N, Lyeb, Moyo S, Nsangou D. (2016). Éducation thérapeutique en vue de la révélation complète du statut aux enfants infectés par le VIH/sida à Yaoundé, Cameroun Acquisitions et compétences. Médecine et Santé Tropicales., 26(3):308-311.
Publisher | Google Scholor























