

Research Article
Determinants of Pneumonia Among Under-Five Children Attending the Public Hospital of Hadiya Zone, Central Ethiopia 2024
1Department of Pediatrics and child health Nursing, College of Medicine and Health sciences, Wachemo University, Hosanna, Ethiopia.
2Departments of midwifery College of Medicine and Health Science, Wachemo University, Hosanna, Ethiopia.
3Departments of comprehensive Nursing College of Medicine and Health Science, Wachemo University, Hosanna, Ethiopia.
*Corresponding Author: Seifu Awgchew, Department of Pediatrics and child health Nursing, College of Medicine and Health sciences, Wachemo University, Hosanna, Ethiopia.
Citation: Awgchew S, Foga S, Gebreselassie R, Ezo E, Zekiwos A. (2025). Determinants of Pneumonia Among Under-Five Children Attending the Public Hospital of Hadiya Zone, Central Ethiopia 2024. Journal of Clinical Paediatrics and Child Health Care, BioRes Scientia Publishers. 3(1):1-9. DOI: 10.59657/2997-6111.brs.26.030
Copyright: © 2026, Seifu Awgchew, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 13, 2025 | Accepted: March 30, 2026 | Published: April 06, 2026
Abstract
Introduction: Pneumonia is an inflammation of the air sacs in the lungs in response to an injury, such as infection. When the airlines also are involved, it could be referred to as bronchopneumonia. It can be one area of the lung or several areas. Approximately 30% of patients with pneumonia are admitted to the hospital. It is the most common associated cause of death in patients with chronic obstructive pulmonary disease (COPD).
Objective: To identify determinants of pneumonia among under-five children who visit under- five OPD in Hadiya Zone public hospitals Central Ethiopia 2024.
Method: An institution-based unmatched case-control research design was used in Hadiya zone public hospitals, with 160 cases and 321 controls of children aged 2-59 months included in the sample. The cases were children with pneumonia, while the controls did not have pneumonia. Ethical clearance was obtained. Data was entered using Epi-Data version 4.6 and analyses using SPSS 27 statistical software, and determinant factors were identified based on P-value less than or equal to 0.05and adjusted odds ratio with 95%CI (AOR).
Result: Place of cooking (AOR: 2.75, 95%CI: 1.66, 4.58), History of Diarrhea in the past 2 weeks (AOR: 6.37, 95%CI: 3.63, 11.2), History of parental asthma in the family (AOR: 4.32, 95%CI: 2.31, 8.05), and a children received PCV vaccine during their infancy period (AOR: 2.09 95%CI: 1.24, 3.51), were found to be determinants of under-five pneumonia.
Conclusion: Globally, the prevalence of pneumonia-related morbidity and death will undoubtedly decline with the widespread use of the Hib and anti-pneumococcal vaccines, along with other proven preventative measures; however, this decline may not be observed in regions where pneumonia remains a major cause of illness and death.
Keywords: under-five pneumonia; determinants; NEMMCSH; public hospitals
Introduction
Pneumonia is an inflammation of the air sacs in the lungs in response to an injury, such as infection. When the airways are also involved, it may be called bronchopneumonia. It can be one area of the lung or several area [1]. According to international data, approximately 30% of the patients with pneumonia are admitted to the hospital It is the predominant related cause of mortality in individuals with chronic obstructive pulmonary disease (COPD).so the burden is expected to increase [2].
Yet over 5 million children are dying every year, and pneumonia accounts for nearly 20% of the deaths. The rate of progress in reducing pneumonia-related mortality has been slower than for other leading causes of child deaths [3]. The World Health Organization data indicates that pneumonia resulted in the deaths of 147,180 children under five years old in 2019, accounting for 22% of all fatalities among children aged 1 to 5 years. The incidence rate of under-five pneumonia is 0.29 episodes per child-year. The developing country accounts for 151.8 million cases per year; of these, 74% are accounted for by fifteen world countries, including Ethiopia [4].
On the other hand, Southeast Asia and Africa are the two continents with the highest rates of under-five pneumonia, reporting an estimated 61 million and 35 million childhood pneumonia cases annually, respectively [5].
Different reports show that from sub-Saharan Africa, Ethiopia has the highest rate of pneumonia, with an estimated 3,370,000 children affected by pneumonia annually [6], and Ethiopia has the fifth-highest under-five child death rate in the world due to pneumonia (62 deaths per 1000) [7]. Based on UNICEF reports, pneumonia accounts for 16 percent of all under-five deaths in sub-Saharan Africa compared to 14% for malaria and 10% for acute diarrheal diseases [8].
Even though some studies have been conducted in Ethiopia on the determinants of under-five pneumonia, they were limited to identifying the hidden risk factors. The burden of pneumonia and lack of information on the practice of early assessment and identification of the problem initiate the need for this study. Also, this study fulfills this gap by assessing the risk factors of pneumonia in a selected governmental hospital of Hadiya zone.
Methods And Materials
Study area and period
The study was conducted in Hadiya zone, which is the capital city of the Central Ethiopia region; also, it is one of the 7 zones in Central Ethiopia. It has 13 woredas and 4 town administrations with a total of 329 kebeles, of which 303 are rural and 26 are urban. It is located 230 Km away from the capital city of Ethiopia. It is situated at an altitude of 1800-2950 meters above sea level and has an average temperature ranging from 10 to 24 degrees centigrade. The zone has 1 specialized hospital and 3 first-level hospitals. This study was conducted in public hospitals of the Hadiya zone from February 1 to March 30, 2024.
Study design
Institutional based un-matched case- control study design was conducted to asses’ determinants of pneumonia among under-five children at public hospital of Hadiya zone Central Ethiopia 2024.
Source population
All under-five children who visit the Hadiya Zone Public Hospital's pediatrics OPD
Study population
All selected under-five children who visited the selected Hadiza zone Public Hospital's pediatrics OPD during the study period
Sample Population
All under-five children who fulfill the inclusion criteria at the selected public hospitals.
Case definition: All under-five children with a diagnosis of pneumonia who come for treatment service during the data collection period
Control definition: all under-five children who visited a 'sick-baby clinic’ and were registered and classified for a condition other than pneumonia within a similar study period.
Inclusion criteria
All under-five children who visited the selected public hospital during the study period.
Exclusion criteria
(Care givers) who did not have any information about the child at the time of data collection
Children who have a cough due to a recent history of liquid and foreign body aspiration
Infants whose age is less than two months.
Sample Size Determination and Sampling Procedure
The sample size is determined using the double population proportion exposure difference formula by considering major determinant variables: number of families, birth to 6 months feeding practice, and the main house without a window. Considering the number of families with more than four as an independent predictor, since it gives the maximum sample size as compared to other exposure variables, which reduces the role of chance? The sample size is determined using Open Epi version 7.2.0.1. The following assumptions were put into consideration: Confidence level of 95%, power of the study 80%, the case-control ratio 1:2, and expected percent of exposures in control and expected percent exposure among cases taken from different studies (Table 1).
Table 1: Sample size determination for determinants of pneumonia among under-five children attending public hospitals in Hadiya zone, Central Ethiopia; hospital-based case-control study, 2024.
| No | Variables | AOR | % Of controls exposed | Total sample Size (Cases +controls) | Ref. |
| 1 | Number of family | 2.1 | 72 | 146+291=437 | (9) |
| 2 | Birth to 6 Months Breastfeeding Practice | 3.3 | 37 | 40+79=119 | (9) |
| 3 | Mainly, a house without windows | 2.42 | 42.43 | 84+101=185 | (10) |
Finally, the maximum sample size is 437(146 cases and 291 controls) after adding a 10% non-respondent rate. 44+437=481(160 cases and 321 controls) was taken for the study.
Sampling procedure
Among the four public hospitals found in the Hadiya zone, two were selected simply randomly. The estimated number of outpatient visits to the under-five children outpatient department of each hospital for two months was counted from registrations and used as a baseline. Then the sample size for each hospital was proportionally allocated. All allocated cases and controls in each hospital will be used as a base to get the sampling fraction. However, the systematic random sampling technique will be used to select both cases and controls for this study. The estimated number of two-month case and control groups was NEMCSH = 240 cases and 710 controls, and Shone 86 cases and 264 controls. To find the sampling fraction of each hospital study population (NEMMCSH), k=710/234=3 for control and k=240/117=2 for case. Shone, k=264/87=3 for control and K=86/43=2 for case, meaning every 3rd member of the control and every 2nd member of the case will be selected. (Figure 1).
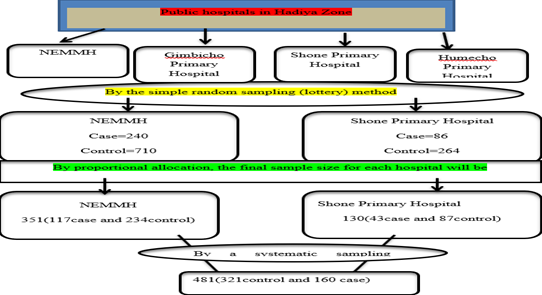
Figure 1: Schematic presentation of sampling procedures followed to get study participants at public hospitals of Hadiya zone, Central Ethiopia, 2024.
Study Variable
Dependent variable
Pneumonia among children under five.
Independent variable
Socio-demographic characteristics (Age of child, Sex of child, Age of the mother, Residence, Education status of mother, Education status of father, Occupation of mother, Occupation of father, Number of less than 5 children in the family, Family size). Child and parental related factors (Diarrhea in the last 2 weeks, URTI in the last 2 weeks, History of parental asthma in the family, A child received pentavalent vaccine, A child received PCV vaccine, A child received measles vaccine, Child HIV status, Malnutrition, Child having repeated attack of pneumonia). House and environmental related factors (Hand washing practice, Fuel used for cooking, Family history of smoking cigarettes, Presence of window in the house, Mother/caregiver carrying child at the back while cooking, Place of cooking, Separate Cattle room).
Data collection instrument and procedures
Parents of children aged two months to five years who were on-site during data collection were eligible to participate in the study. Face-to-face interviews and document review will be done to collect data on socio-demographic and independent variables. The data from mothers/caregivers will be collected by using a pretested, structured, and interviewer-administered questionnaire, which is adapted from different literature [9-12]. The physician examined the patients as cases and controls based on physical examination and chest X-ray results. The data collection process was conducted individually at a convenient location for the respondents. All information was collected on a data collection sheet designed for the study.
Data quality control
The questionnaire was evaluated by experts in related fields. Intensive training that lasts two days was offered by the principal investigator to the data collectors and supervisors on the technique of timely data collection, the purpose of data collection, the contents of the questionnaires, how to approach the respondents, how to deal with difficulties that may arise during the data collection phase, and the issue of confidentiality and privacy. The data collection instrument was pretested on 5% of the sample. Finally, all the collected data was also checked by the supervisor and investigator for its completeness and consistency.
Data processing and analysis
Data was entered using Epi-Data version 4.6 and analyzed using SPSS 27 statistical software. The regression model assumption was checked using a goodness-of-fit test, such as Hosmer, to identify and exclude variables that cause poor fit in the model. A bivariate regression model was fitted for each explanatory variable. Accordingly, those variables having a p-value less than or equal to 0.05 in the bivariate analysis were fitted to the multivariable logistic regression model. In multivariable regression, a P-value less than or equal to 0.05 was considered statistically significant. Multi-collinearity among independent variables was checked by the variance inflation factor (VIF).
Results
Socio-demographic characteristics of the respondents
The study has involved all mothers with their children who gave their consent (response rate of 100%). Of this, 73 (45.6%) of cases and 143 (44.5%) of controls were permanently rural residences. The mothers who participated in the study had an average age of 28.69 (SD ±4.94) for cases and 27.96 (SD ±5.87) for control. In contrast, the mean age of children in the study was 26.73 (SD ±17.43) months for cases and 19.9 (SD ±14.22) months for control, respectively (Table 2, Figure 2).
Table 2: Socio-Demographic Characteristics of the Participants at Public Hospitals of Hadiya Zone, Central Ethiopia, 2024
| Variable (N=481) | Category | Case (N=160) | Control (N=321) | |
| Percent | Frequency | Percent | ||
| Age of the mother | 18-26 | 11.9 | 109 | 34 |
| 27-35 | 58.8 | 145 | 45.2 | |
| >=36 | 29.4 | 67 | 20.9 | |
| Educational status of the mother | No formal education | 18.1 | 70 | 21.8 |
| Primary | 37.5 | 124 | 38.6 | |
| Secondary | 25.6 | 88 | 27.4 | |
| Higher education | 18.8 | 39 | 12.1 | |
| Residence | Rural | 45.6 | 143 | 44.5 |
| Urban | 54.4 | 178 | 55.5 | |
| Educational status of father | No formal education | 10.6 | 76 | 23.7 |
| Primary | 33.8 | 103 | 32.1 | |
| Secondary | 24.4 | 80 | 24.9 | |
| Higher education | 31.3 | 62 | 19.3 | |
| Occupation status of mother | House wife | 70 | 137 | 42.7 |
| farmer | 8.1 | 107 | 33.3 | |
| Government | 15.6 | 49 | 15.3 | |
| Merchant | 6.3 | 28 | 8.7 | |
| Occupation status of father | Farmer | 41.9 | 123 | 38.3 |
| Government | 31.3 | 112 | 34.9 | |
| Merchant | 26.9 | 86 | 28.8 | |
| Age of the child | 2monthe – 11month | 10 | 92 | 28.7 |
| 12month – 27month | 48.1 | 145 | 45.2 | |
| 28 months – 59 months | 41.9 | 84 | 26.2 | |
| Sex of the child | Male | 45 | 166 | 51.7 |
| Female | 55 | 155 | 48.3 | |
| Family size | More than four | 57.5 | 136 | 42.4 |
| Less than or equal to 4 | 42.5 | 185 | 57.6 | |
Figure 2: Children's mothers' occupational frequency distribution found in public hospitals of Hadiya Zone, Central Ethiopia.
House and Environmental Characteristics of the Participants
About 44 (27.5%) of the case population and 177 (55.1%) of the control population used charcoal/wood for cooking purposes. More than fifty percent (91, 56.9%) of the cases and 151 (47%) of the control children had a family history of cigarette smoking. Nearly equal proportions of the cases, 45% and 46.1% of control participants, lived in a house without a window (Table 3).
Table 3: House and Environmental Characteristics of the Respondents at Public Hospitals of Hadiya Zone, Central Ethiopia 2024.
| Variable (N=481) | Category | Case (N=160) | Control (N=321) | ||
| Frequency | Percent | Frequency | Percent | ||
| Diarrhea in the last 2 weeks | Yes | 20 | 12.5 | 154 | 48 |
| No | 140 | 87.5 | 167 | 52 | |
| URTI in the last 2 weeks | Yes | 81 | 50.6 | 155 | 48.3 |
| No | 79 | 49.4 | 166 | 51.7 | |
| History of parental asthma in the family | Yes | 21 | 13.1 | 135 | 42.1 |
| No | 139 | 86.9 | 186 | 57.9 | |
| A child received the Pentavalent vaccine | Yes | 81 | 50.6 | 175 | 54.5 |
| No | 79 | 49.4 | 146 | 45.5 | |
| A child received the PCV vaccine | Yes | 122 | 76.3 | 180 | 56.1 |
| No | 38 | 23.7 | 141 | 43.9 | |
| A child received the measles vaccine | Yes | 74 | 46.3 | 146 | 45.5 |
| No | 86 | 53.7 | 175 | 54.5 | |
| Child HIV status | Negative | 153 | 95.6 | 314 | 97.8 |
| Positive | 7 | 4.4 | 7 | 2.2 | |
| The weight for height of a child | Wasted (≤ -2 SD) | 29 | 18.1 | 82 | 25.5 |
| Normal (≥ -2 SD) | 131 | 81.9 | 239 | 74.5 | |
| The weight for age of the child | Underweight (≤ -2 SD) | 26 | 16.3 | 98 | 30.5 |
| Normal (≥ -2 SD) | 134 | 83.7 | 223 | 69.5 | |
| A child having repeated attacks of pneumonia | Yes | 52 | 32.5 | 100 | 31.2 |
| No | 108 | 67.5 | 221 | 68.8 | |
| Birth to 6 Months Breastfeeding Practice | Non exclusive | 63 | 39.4 | 129 | 40.2 |
| Exclusive | 97 | 60.6 | 192 | 59.8 | |
Parental and Child-Related Characteristics
Of all under-five children included in the study, 20(12.5%) of cases and 154(48%) of controls had a history of diarrhea in the last two weeks. More than half of the cases, 81(50.6%), and control 175 (54.5%) of children received their pentavalent vaccine. Similarly, 122(76.3%) of cases and 180(56.1%) of controls received the PCV vaccine (Table 4, Figure 3).
Table 4: Parental and Children Related Characteristics of Respondents at Public hospitals of Hadiya zone, Central Ethiopia 2024.
| Variable (N=481) | Category | Case (N=160) | Control (N=321) | ||
| Frequency | Percent | Frequency | Percent | ||
| Diarrhea in the last 2 weeks | Yes | 20 | 12.5 | 154 | 48 |
| No | 140 | 87.5 | 167 | 52 | |
| URTI in the last 2 weeks | Yes | 81 | 50.6 | 155 | 48.3 |
| No | 79 | 49.4 | 166 | 51.7 | |
| History of parental asthma in the family | Yes | 21 | 13.1 | 135 | 42.1 |
| No | 139 | 86.9 | 186 | 57.9 | |
| A child received the Pentavalent vaccine | Yes | 81 | 50.6 | 175 | 54.5 |
| No | 79 | 49.4 | 146 | 45.5 | |
| A child received the PCV vaccine | Yes | 122 | 76.3 | 180 | 56.1 |
| No | 38 | 23.7 | 141 | 43.9 | |
| A child received the measles vaccine | Yes | 74 | 46.3 | 146 | 45.5 |
| No | 86 | 53.7 | 175 | 54.5 | |
| Child HIV status | Negative | 153 | 95.6 | 314 | 97.8 |
| Positive | 7 | 4.4 | 7 | 2.2 | |
| The weight for height of a child | Wasted (≤ -2 SD) | 29 | 18.1 | 82 | 25.5 |
| Normal (≥ -2 SD) | 131 | 81.9 | 239 | 74.5 | |
| The weight for age of the child | Underweight (≤ -2 SD) | 26 | 16.3 | 98 | 30.5 |
| Normal (≥ -2 SD) | 134 | 83.7 | 223 | 69.5 | |
| A child having repeated attacks of pneumonia | Yes | 52 | 32.5 | 100 | 31.2 |
| No | 108 | 67.5 | 221 | 68.8 | |
| Birth to 6 Months Breastfeeding Practice | Non exclusive | 63 | 39.4 | 129 | 40.2 |
| Exclusive | 97 | 60.6 | 192 | 59.8 | |
Figure 3: PCV vaccine Frequency Distribution among Under-five Children at public hospitals of Hadiya Zone, Central Ethiopia
Determinants of Under-five Pneumonia
Binary logistic regression analysis was utilized to uncover independent factors of pneumonia in children under the age of five. First, the respondents' socio-demographic variables, housing, and environmental variables, as well as parent- and child-related characteristics, were compared to the outcome variable, which is a risk factor, using a bivariate analysis. Variables having a P-value less than or equal to 0.05 were fitted into the final binary logistic regression model (multivariable analysis). As a result, place of cooking (AOR: 2.75, 95% CI: 1.66, 4.58), history of diarrhea in the past 2 weeks (AOR: 6.37, 95% CI: 3.63, 11.2), history of parental asthma in the family (AOR: 4.32, 95% CI: 2.31, 8.05), and children receiving the PCV vaccine during their infancy period (AOR: 2.09, 95% CI: 1.24, 3.51) were significantly associated with under-five-year-old pneumonia (Table 5).
Table 5: Bivariable and multivariable analysis of pneumonia among under-five-year children at public hospitals of Hadiya zone, Central Ethiopia 2024.
| Variable (N=481) | Category | Under-five pneumonia | COR (95%CI) | AOR (95%CI) | P-value | |
| Case (n=160) | Control (n=321) | |||||
| Residence | Rural | 73(15.2%) | 143(29.72%) | 1.959(1.48,2.9) | 0.88(0.57,1.37) | 0.56 |
| Urban | 87(18.08%) | 178((37%) | 1 | 1 | ||
| Sex of the child | Female | 88((18.29%) | 166(34.51%) | 1.141(1.35,2.9) | 0.86(0.46,1.02) | 0.67 |
| Male | 72(14.96%) | 155(32.22%) | 1 | 1 | ||
| Presence of a window in the house | Yes | 88(18.29%) | 173((35.96%) | 1 | 1 | 0.089 |
| No | 72(14.96%) | 148(30.76%) | 1.05(1.55,2.72) | 0.65(0.4,1.06) | ||
| Place of cooking | In kitchen | 120(24.94%) | 162(33.68%) | 1 | 1 | 0.001 |
| In house | 40(8.31%) | 159(33.05%) | 3.1(2.81,5.62) | 2.75(1.66,4.58) | ||
| Diarrhea in the last 2 weeks | Yes | 20(4.15%) | 154(32.01%) | 6.5(4.83,12.26) | 6.37(3.63,11.2) | 0.001 |
| No | 140(29.10%) | 167(34.72%) | 1 | 1 | ||
| URTI in the last 2 weeks | Yes | 81(16.83%) | 155(32.22) | 1.214(1.46,2.5) | 0.82(0.53,1.28) | 0.39 |
| No | 79(16.42%) | 166(34.51%) | 1 | 1 | ||
| History of parental asthma in the family | Yes | 21(4.36%) | 135(28.06%) | 5(4.01,10.2) | 4.32(2.31,8.05) | 0.001 |
| No | 139(28.89%) | 186(38.67%) | 1 | 1 | ||
| A child received the PCV vaccine | Yes | 122(25.36%) | 180(37.42%) | 1 | 1 | 0.005 |
| No | 38(7.9%) | 141(29.31%) | 2.51(2.6,5.3) | 2.09(1.24,3.51) | ||
| The weight for height of a child | Wasted (≤ -2 SD) | 29(6.02%) | 82(17.04%) | 2.0(1.85,4.31) | 0.55(0.29,1.04) | 0.06 |
| Normal (≥ -2 SD) | 131(27.23%) | 239(49.68%) | 1 | 1 | ||
| A child having repeated attacks of pneumonia | Yes | 52(10.81%) | 100(20.79%) | 1.62(1.37,2.68) | 0.61(0.36,1.02) | 0.061 |
| No | 108(22.45%) | 221(45.94%) | 1 | 1 | ||
| Birth to 6 Months Breastfeeding Practice | Non exclusive | 63(13.09%) | 129(26.81%) | 2.04(1.51,2.76) | 0.82(0.5,1.33) | 0.42 |
| Exclusive | 97(20.16%) | 192(39.9%) | 1 | 1 | ||
Discussion
Pneumonia in children under the age of five is a prominent cause of illness and death globally, with particularly high rates in impoverished countries such as Ethiopia. Understanding the determining variables is critical for developing an effective care and preventive approach for pediatric pneumonia. These studies identify easy-to-prevent determining variables. So, the result of this study identifies that the place of cooking, diarrhea in the last 2 weeks, history of parental asthma in the family, and children who received the PCV vaccine during their infancy period were significant factors associated with under-five pneumonia.
The place of cooking was the key variable that indicates association with under-five pneumonia; children whose mothers cook in the living room were 2.75 times more likely to be affected by pneumonia than those whose mothers cook in the kitchen. Similar studies in Indonesia, East Africa, a systematic review in, Ethiopia, and a study conducted in Worabe, Ethiopia, respectively, support this result [6,13-15]. This could be due to indoor pollution from unsafe energy sources such as charcoal, wood, and biomass. Indoor air pollution, notably from the use of solid fuels for cooking and heating, is a major risk factor for childhood pneumonia, particularly in nations with low- and moderate-income levels like Ethiopia. Exposure to these pollutants weakens a child's respiratory system, leaving them more susceptible to diseases like pneumonia. Reducing indoor air pollution through initiatives like encouraging clean fuel usage and better cooking stoves is critical for pneumonia prevention.
The odds of children who had diarrhea in the past two weeks were 6.37 times more likely to acquire pneumonia than children who did not have diarrhea during the same period. This study was consistent with other previous studies in Brazil, Kenya, Gambela, Ethiopia and Gonder, Ethiopia, respectively [10,11,16,17]. The possible reason may be due to the fact that the history of diarrhea is strongly associated with the development of pneumonia in children under five, and diarrhea is one of the main causes of mortality in this age range. This elevated risk is probably brought on by a compromised immune system as well as other elements associated with inadequate sanitation and hygiene. Consequently, in order to lessen the burden of these infectious diseases, important preventative strategies include rotavirus vaccine, hand washing with soap, access to safe drinking water, better sanitation, and exclusive breastfeeding for the first six months.
The finding of this study indicates that a history of parental asthma in the family was strongly associated with pneumonia in children. This finding agreed with studies conducted in different parts of the world: the Philippines, the Netherlands, and Worabe, Ethiopia, respectively [15,18,19]. The possible explanation might be that an important risk factor for pediatric pneumonia is a history of parental asthma; research suggests that children who have asthmatic parents are at a higher risk of contracting pneumonia themselves. Common genetic predispositions and environmental variables that promote vulnerability to both illnesses are probably the cause of this connection. Genetic factors can impact both pneumonia and asthma. A child who has an asthmatic parent may inherit genes that increase their vulnerability to respiratory conditions like pneumonia. Children who suffer from asthma or pneumonia are more susceptible to respiratory infections since these conditions can impact immune system development and function.
The PCV vaccine was also another factor identified to affect the occurrence of pneumonia in children under five years old. Children who didn’t receive the PCV vaccine were twofold [2.09 [1.24, 3.51] more affected by pneumonia than those who received the PCV vaccine. Those similar studies done in different countries, like the Public Health Foundation of India, state systematic reviews in East Africa and at Jimma University Medical Center in Ethiopia, respectivel [6,20,21]. support the finding. This association might be Immunization mitigates childhood pneumonia through two mechanisms. Firstly, vaccinations avert infections that directly induce pneumonia, such as Homophiles influenza type B, and infections like measles and pertussis that can indicate pneumonia as a complication can also be avoided by vaccination. On the other hand, PCV functions via boosting the immunological system to generate antibodies against the Streptococcus pneumonia bacterium, a prevalent cause of pneumonia. PCV has demonstrated considerable efficacy in decreasing the occurrence of pneumococcal pneumonia in children, with research indicating substantial decreases. The vaccination further safeguards against other serious pneumococcal infections such as meningitis and sepsis, which can be life-threatening in hospitalized patients and in situations of radiological confirmed pneumonia. PCV has significantly reduced pneumonia-related fatalities in children by preventing pneumococcal pneumonia.
Limitation of the study
The study did not take into account private healthcare institutions or the entire population, and the diagnosis of pneumonia was based on the clinical WHO IMNCI categorization rules, which created misclassification and recall bias. The severity of pneumonia risk factors was not examined in the study, nor was it connected to outcomes like survival, pediatric morbidity, or length of stay in the hospital.
Conclusion and Recommendation
Globally, the prevalence of pneumonia-related morbidity and death will undoubtedly decline with the widespread use of the Hib and anti-pneumococcal vaccines, along with other proven preventative measures; however, this decline may not be observed in regions where pneumonia remains a major cause of illness and death. The prognosis of these children can be greatly improved by placing a strong emphasis on early identification of risk factors that are known to be locally or globally linked with a poor result and the development of an appropriate case management strategy. It is recommended that all healthcare facilities provide health education on vaccinations and ways to reduce indoor pollution, as well as early treatment and prevention of diarrhea and chronic lower respiratory infections in children.
Abbreviations
AURTI: Acute upper respiratory tract infection; COPD: chronic obstructive pulmonary disease; CMR, child mortality rate; EDHS: Ethiopian Demographic and Health Survey; MDG: millennium developmental goal, SDG: Sustainable Development Goal, UNICEF: United Nations Children’s Fund, WHO: World Health Organization.
Declarations
Ethical consideration
Ethical clearance was obtained from Wachemo University College of medicine and health science and approved by Wachemo university institutional review board (WCU/IRB/0039/24) and a formal letter of cooperation to conduct this research was written to select Hadiya Zone Public Hospitals. Thoroughly, our research passed required the principles of the declaration of the Helsinki General Assembly, Seoul, Korea, and October 2008.
Acknowledgment
We would like to thank the study participants for the scarification of their valuable time spent filling out questionnaires, selected Hadiya Zone Public Hospitals, and Wachemo university.
Informed consent
Written informed consent was obtained from each participant nurses, and the information obtained from them would not have been disclosed. Coding was used to eliminate names and other personal identification of respondents to ensure anonymity, privacy, and confidentiality.
Competing of interests
All authors declare that they have no conflict of interest.
Funding
This research didn’t receive any grant from any funding agency in the public, commercial or not-for-profit sectors.
Clinical Trail
Not applicable
Authors` contribution
All authors have made substantial contributions to the work. Participated in the conception, design, and acquisition, conducted the data analysis and interpretation; took part in drafting, revising, and critically reviewing the article. All authors gave final approval of the version to be published and all authors have agreed on the journal to which the article has been submitted; agreed to be personally accountable for all aspects of the work.
References
- Series I. (2020). ATS Patient Education Series © 2016 American Thoracic Society Online version updated October 2020 Am J Respir Crit Care Med Vol. 193, P1-P2, 2016. Am Thorac Soc., 193:2016.
Publisher | Google Scholor - Chung Y, Morgan L. (2015). Pneumonia: Who is at risk in your practice? Med Today., 16(8):35–42.
Publisher | Google Scholor - (2021). The Pneumonia WHO and UNICEF integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD) aims to accelerate pneumonia control with a combination of interventions to protect, prevent, and treat pneumonia in children.
Publisher | Google Scholor - Unicef Stc. (2019). Every Child’ S Right to Survive: An Agenda to End Pneumonia Deaths.
Publisher | Google Scholor - Chen J, Hu P, Zhou T, Zheng T, Zhou L. et al. (2018). Epidemiology and clinical characteristics of acute respiratory tract infections among hospitalized infants and young children in Chengdu, West China, 2009-2014. BMC Pediatr.; 18(1):1–8.
Publisher | Google Scholor - Abate BB, Kasie AM, Reta MA, Kassaw MW. (2020). Neonatal sepsis and its associated factors in East Africa: a systematic review and meta-analysis. Int J Public Health., 65(9):1623–1633.
Publisher | Google Scholor - Morris SS, Black RE, Tomaskovic L. (2003). Predicting the distribution of under-five deaths by cause in countries without adequate vital registration systems. Int J Epidemiol., 32(6):1041–1051.
Publisher | Google Scholor - Pires SM, Fischer-Walker CL, Lanata CF, Devleesschauwer B, Hall AJ, et al. (2015). Aetiology-specific estimates of the global and regional incidence and mortality of diarrhoeal diseases commonly transmitted through food. PLoS One., 10(12):1–17.
Publisher | Google Scholor - Ewnetu H. (2016). Determinants of Community Acquired Pneumonia among Children in Kersa District, Southwest Ethiopia: Facility Based Case Control Study. J Pediatr Neonatal Care., 5(2):1–7.
Publisher | Google Scholor - Getahun A, Alemayehu S, Ayalew K. (2022). Determinants of Community-Acquired Pneumonia among under-Five Children in Tehulederie District, Northeast Ethiopia. Int J Pediatr Res., 8(1):1–9.
Publisher | Google Scholor - Bazie GW, Seid N, Admassu B. (2020). Determinants of community acquired pneumonia among 2 to 59 months of age children in Northeast Ethiopia: a case-control study. Pneumonia., 12(1).
Publisher | Google Scholor - Markos Y, Dadi AF, Demisse AG, Ayanaw Habitu Y, Derseh BT, et al. (2019). Determinants of under-five pneumonia at Gondar University Hospital, Northwest Ethiopia: An unmatched case-control study. J Environ Public Health.
Publisher | Google Scholor - Sutriana VN, Sitaresmi MN, Wahab A. (2021). Risk factors for childhood pneumonia: a case-control study in a high prevalence area in Indonesia. Clin Exp Pediatr., 64(11):588–595.
Publisher | Google Scholor - Alamneh YM, Adane F. (2020). Magnitude and Predictors of Pneumonia among Under-Five Children in Ethiopia: A Systematic Review and Meta-Analysis.
Publisher | Google Scholor - Seramo R kumdin, Awol SM, Wabe YA, Ali MM. (2022). Determinants of pneumonia among children attending public health facilities in Worabe town. Sci Rep., 12(1):1–9.
Publisher | Google Scholor - Fonseca Lima EJ da, Mello MJG, Albuquerque M de FPM de, Lopes MIL, Serra GHC, et al. (2016). Risk factors for community-acquired pneumonia in children under five years of age in the post-pneumococcal conjugate vaccine era in Brazil: A case control study. BMC Pediatric.16(1):1–9.
Publisher | Google Scholor - Onyango D, Kikuvi G, Amukoye E, Omolo J. (2012). Risk factors of severe pneumonia among children aged 2-59 months in western Kenya: A case control study. Pan Afr Med J., 13:1–13.
Publisher | Google Scholor - Kosai H, Tamaki R, Saito M, Tohma K, Alday PP. (2015). Incidence and Risk Factors of Childhood Pneumonia-Like Episodes in Biliran Island., 1–19.
Publisher | Google Scholor - Review AS, The ON, Of B, Diarrhoea ON, Mortality P. Short-term effects of breastfeeding.
Publisher | Google Scholor - Jackson S, Kyle H, Pulanić D, Campbell H. (2013). Risk factors for severe acute lower respiratory infections in children – a systematic review and meta-analysis., 110–121.
Publisher | Google Scholor - Tegenu K, Geleto G, Tilahun D, Bayana E, Bereke B. (2022). Severe pneumonia: Treatment outcome and its determinant factors among under-five patients, Jimma, Ethiopia. SAGE Open Med., 10.
Publisher | Google Scholor























