

Research Article
Cellular Responses and Cell Death Induced by Diagnostic and Interventional X-Ray Exposures: A Systematic Review of Human Clinical and Biological Evidence with Implications for Radiation Protection
Department of Physics with Electronics. Federal University. Birnin Kebbi, Nigeria.
*Corresponding Author: Buhari Samaila, Department of Physics with Electronics. Federal University. Birnin Kebbi, Nigeria.
Citation: Samaila B. (2026). Cellular Responses and Cell Death Induced by Diagnostic and Interventional X-Ray Exposures: A Systematic Review of Human Clinical and Biological Evidence with Implications for Radiation Protection, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 6(6):1-12. DOI: 10.59657/2997-6103.brs.26.131
Copyright: © 2026 Buhari Samaila, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 23, 2026 | Accepted: April 14, 2026 | Published: April 20, 2026
Abstract
Background: Diagnostic and interventional X-ray procedures are indispensable in modern medicine; however, increasing evidence suggests that even low-dose exposures may induce measurable biological effects at the cellular level. While these procedures typically deliver doses below established deterministic thresholds, concerns persist regarding radiation-induced apoptosis, cytotoxicity, and genotoxicity in radiosensitive human tissues. Understanding these effects is essential for strengthening radiation protection, optimization strategies, and diagnostic reference level (DRL) frameworks.
Objective: This systematic review aimed to critically synthesize human clinical evidence on cellular responses and cell death induced by diagnostic and interventional X-ray exposures, with particular emphasis on hematological cells, oral/buccal epithelial cells, pediatric sensitivity, and dose–response relationships relevant to radiation protection.
Materials and Methods: A systematic literature review was conducted in accordance with PRISMA 2020 guidelines. Comprehensive searches were performed across PubMed/MEDLINE, Scopus, Web of Science, EMBASE, and Google Scholar from inception to December 2025. Eligible studies were peer-reviewed human clinical investigations reporting diagnostic or interventional X-ray exposure with measurable cellular outcomes, including apoptosis, mitochondrial depolarization, cytotoxicity, or DNA damage. Two reviewers independently screened records, extracted data, and resolved discrepancies by consensus. Due to methodological heterogeneity, a narrative synthesis was undertaken.
Results: Out of 449 identified records, 45 human clinical studies met the inclusion criteria and were synthesized. Studies spanned Asia, Europe, the Americas, and Australia, encompassing adult and pediatric populations. Diagnostic procedures included dental radiography, panoramic radiography, digital lateral radiography, conventional diagnostic X-ray imaging, and contrast-enhanced examinations. Reported absorbed doses predominantly ranged from 0.01 to 0.5 mGy per examination. Across studies, hematological cells (lymphocytes and leukocytes) consistently demonstrated apoptosis, mitochondrial membrane depolarization, and oxidative stress, even at doses below 0.1 mGy. Oral and buccal epithelial cells exhibited cytotoxic changes such as karyolysis, pyknosis, and micronucleus formation. Pediatric populations showed greater magnitudes of cell death at comparable doses, indicating heightened radiosensitivity. Interventional and contrast-enhanced procedures demonstrated dose-amplification effects, with increased DNA damage and reduced cell survival.
Conclusion: This systematic review provides robust clinical evidence that diagnostic X-ray exposures are not biologically inert, even at sub-milligray dose levels. Measurable cell death-predominantly apoptosis-occurs across multiple human tissues, with amplified effects in pediatric populations and contrast-enhanced procedures. These findings support the biological plausibility of stochastic effects at diagnostic doses and are consistent with the linear no-threshold model. Strengthened justification, optimization, and strict adherence to DRL- and ALARA-based practices are essential to minimize cumulative biological risk, particularly in vulnerable populations.
Keywords: diagnostic x-ray imaging; low-dose ionizing radiation; apoptosis; cytotoxicity; pediatric radiosensitivity; contrast-enhanced imaging; radiation protection
Introduction
Medical X-ray imaging has become an indispensable component of modern healthcare, playing a critical role in disease diagnosis, treatment planning, and clinical decision-making. Diagnostic procedures such as dental radiography, panoramic imaging, digital lateral radiography, and conventional X-ray examinations are widely regarded as low-dose modalities and are routinely performed across all age groups. Despite their clinical benefits, these procedures expose patients to ionizing radiation, raising persistent concerns regarding potential biological effects at low dose levels. International radiation protection frameworks emphasize that no level of ionizing radiation exposure can be considered entirely risk-free, particularly when exposures are repeated or involve radiosensitive populations (ICRP, 2007; Shi & Tashiro, 2018). At the cellular level, ionizing radiation deposits energy that can initiate a cascade of biological events, including DNA strand breaks, oxidative stress, mitochondrial dysfunction, and activation of programmed cell death pathways. Apoptosis represents a central mechanism through which damaged cells are eliminated, thereby maintaining tissue integrity. While high-dose radiation effects are well characterized, the biological consequences of low-dose diagnostic X-ray exposure remain an area of active scientific debate. Emerging evidence suggests that even sub-milligray doses may elicit measurable cellular responses, challenging the long-held assumption that diagnostic exposures are biologically negligible (Tungjai et al., 2017; Supawat et al., 2021).
Human clinical studies have increasingly reported evidence of apoptosis, cytotoxicity, and mitochondrial membrane depolarization in hematological cells, particularly lymphocytes and leukocytes, following routine diagnostic X-ray examinations. These cells are recognized as sensitive biomarkers of radiation exposure due to their rapid turnover and high proliferative capacity. Investigations involving blood samples from exposed patients have demonstrated oxidative stress responses and early apoptotic signaling at absorbed doses below 0.1 mGy, indicating a measurable biological impact even at ultra-low exposure levels (Tungjai et al., 2017; Letechipia et al., 2023). Similarly, oral and buccal epithelial cells have been extensively studied as non-invasive indicators of radiation-induced cytotoxicity. Dental and panoramic radiographic procedures have been associated with increased frequencies of karyolysis, pyknosis, and micronucleus formation in exfoliated oral mucosa cells of both adults and children (Ribeiro & Angelieri, 2008; Li et al., 2018). These cytological changes reflect underlying apoptotic and necrotic processes and provide clinically relevant evidence that routine dental imaging can induce transient but detectable cellular injury. Of particular concern is the heightened radiosensitivity of pediatric populations, attributable to higher cell proliferation rates, longer post-exposure life expectancy, and less efficient DNA repair mechanisms. Studies focusing on children undergoing panoramic dental radiography consistently demonstrate greater magnitudes of cell death and cytotoxic biomarkers compared to adults exposed to similar diagnostic doses (Angelieri et al., 2007). These findings underscore the need for pediatric-specific radiation protection strategies and reinforce the importance of justification and optimization in pediatric imaging.
In addition to standard diagnostic procedures, interventional and contrast-enhanced X-ray examinations introduce further complexity by increasing localized radiation dose and biological effectiveness. Evidence indicates that iodinated contrast media can amplify radiation-induced DNA damage and reduce cellular survival, even when physical dose levels remain within diagnostic ranges (Tokita et al., 1990; Harbron et al., 2017). Moreover, chronic low-dose occupational exposure among interventional radiologists has been associated with adaptive cellular responses accompanied by persistent biological stress, highlighting cumulative exposure concerns (Russo et al., 2012). Given the growing body of human clinical evidence demonstrating measurable cellular effects at diagnostic dose levels, a systematic synthesis of these findings is warranted. This review therefore aims to critically evaluate human clinical studies reporting cell death and cytotoxic responses induced by diagnostic and interventional X-ray exposures, with emphasis on hematological and epithelial tissues. By integrating evidence across populations, procedures, and dose ranges, the review seeks to strengthen the biological basis for radiation protection principles, including the ALARA concept, diagnostic reference levels (DRLs), and age-specific optimization strategies.
Materials and Methods
Study Design
This study was a systematic literature review conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Page et al., 2021). The review aimed to synthesize evidence on cellular responses and cell death induced by diagnostic X-ray procedures, including dental radiography, panoramic radiography, digital lateral radiography, and conventional X-ray imaging in human populations. Primary outcomes included apoptosis, mitochondrial depolarization, cytotoxicity, and genotoxic markers in hematological and epithelial cells.
Eligibility Criteria
Inclusion Criteria: Human clinical studies assessing cellular responses (apoptosis, cytotoxicity, DNA damage) following diagnostic X-ray exposure, Studies reporting quantitative or qualitative measures of cell death in hematological cells (lymphocytes, leukocytes) or oral/buccal epithelial cells, Studies reporting absorbed doses or estimated X-ray exposure, typically less than 1 mGy, Peer-reviewed articles published in English, with full-text availability.
Exclusion Criteria: Studies without measurable cell death or cytotoxicity endpoints, Reviews, commentaries, editorials, and conference abstracts lacking original data, Studies assessing non-diagnostic radiation sources or therapeutic X-ray doses.
Information Sources and Search Strategy
A comprehensive literature search was conducted in the following electronic databases from inception to December 2025: PubMed/MEDLINE, Web of Science, Scopus, EMBASE, Google Scholar, researchgate, Academia and other Journals websites. Search terms were formulated using Boolean operators and Medical Subject Headings (MeSH) to capture studies on diagnostic X-rays and cellular endpoints: ("diagnostic X-ray" OR "dental radiography" OR "panoramic radiography" OR "digital lateral radiography”) AND ("cell death" OR "apoptosis" OR "cytotoxicity" OR "mitochondrial depolarization" OR "DNA damage") AND ("human" OR "clinical study"). The search was limited to English language with no restriction on publication year.
Study Selection
The PRISMA protocol was followed. Identified records were imported into excel spreadsheet for duplicate removal. Titles and abstracts were screened independently by two reviewers to identify studies meeting inclusion criteria. Full texts of potentially eligible studies were retrieved and assessed. Discrepancies were resolved by discussion or consultation with a third reviewer.
Data Extraction
A standardized data extraction form was used to collect information from each study: Author(s) and year of publication, Geographic location, Study design and population (adult/pediatric), Diagnostic modality and absorbed dose (mGy), Type of cells assessed (hematological or epithelial), Method of cell death detection (flow cytometry, cytology, staining, etc.), Key findings (apoptosis, mitochondrial depolarization, cytotoxicity) and Reported gaps and limitations. Data extraction was performed independently by two reviewers and cross-verified for accuracy. A PRISMA Protocol was followed to illustrate the identification, screening, and inclusion of studies.
Data Synthesis
Due to heterogeneity in cell types, doses, and detection methods, a narrative synthesis was conducted rather than a meta-analysis. Findings were grouped according to cell type (hematological vs epithelial), population age (adult vs pediatric), and dose range. Key trends in apoptosis, cytotoxicity, and dose-response relationships were summarized. Evidence was interpreted in the context of low-dose radiation biological plausibility, referencing the linear no-threshold model (ICRP, 2007; Shi & Tashiro, 2018).
Results
Diagnostic X-ray Exposures and Cell Death
Across the studies examining diagnostic X-ray exposures, a consistent pattern emerges indicating that even low-dose procedures can induce measurable cellular stress and cytotoxicity. In vitro and ex vivo analyses, such as those by Anoopkumar-Dukie et al. (2005) and Tungjai et al. (2017), show that conventional diagnostic X-rays and radiography trigger oxidative stress, DNA damage, mitochondrial depolarization, cell-cycle arrest, and apoptosis in lymphocytes and leukocytes, suggesting that sub-lethal injury and programmed cell death occur even at routine diagnostic doses. Dental and panoramic radiography studies (Ribeiro & Angelieri, 2008; Angelieri et al., 2007; Li et al., 2018) similarly report increased apoptosis, karyolysis, and cytotoxicity in buccal and oral mucosa cells, with pediatric populations demonstrating heightened radiosensitivity, emphasizing tissue-specific vulnerability. Evidence from digital dental radiography (Ribeiro et al., 2011) indicates that cell death can occur without persistent genotoxic effects, suggesting transient cytotoxic responses. Despite these findings, several gaps remain, including small sample sizes, short-term follow-up, absence of detailed dose reconstruction, limited apoptosis pathway analysis, and insufficient assessment of long-term recovery and cumulative effects. Collectively, these studies indicate that diagnostic X-rays, while generally safe, are biologically active at the cellular level, highlighting the need for careful dose optimization, monitoring, and further research to quantify cell death thresholds and elucidate long-term cellular outcomes.
Table 1: Diagnostic X-ray Procedures and Evidence of Cell Death.
| Author (Year) | Location | Paper Title | Diagnostic Modality | Method | Key Findings | Conclusion | Gaps |
| Anoopkumar-Dukie et al. (2005) | Australia | Further evidence for biological effects resulting from ionizing radiation doses in the diagnostic X-ray range | Conventional diagnostic X-ray | In-vitro lymphocyte assays | Oxidative stress and DNA damage observed at diagnostic doses | Diagnostic X-rays induce sub-lethal cellular injury | Cell death endpoints not fully quantified |
| Tungjai et al. (2017) | Thailand | Effects of medical diagnostic low-dose X rays on human lymphocytes | Diagnostic radiography | Human blood samples | Apoptosis, mitochondrial depolarization, cell-cycle arrest | Diagnostic X-rays can induce apoptotic cell death | Limited population size |
| Letechipia et al. (2023) | Mexico | Apoptosis and cellular stress induction in human leukocytes by dental X-rays | Dental radiography | Leukocyte biomarkers | Increased apoptosis and oxidative stress | Dental X-rays induce leukocyte cell death | Short-term follow-up |
| Ribeiro & Angelieri (2008) | Brazil | Cytogenetic biomonitoring of oral mucosa cells from adults exposed to dental X-rays | Dental X-ray | Buccal micronucleus assay | Cytotoxicity and increased karyolysis | Diagnostic dental X-rays cause cell loss | No apoptosis pathway analysis |
| Angelieri et al. (2007) | Brazil | DNA damage and cellular death in oral mucosa cells of children | Panoramic dental radiography | Pediatric buccal cell analysis | Increased apoptosis and cell death markers | Children show higher radiosensitivity | Dose reconstruction absent |
| Li et al. (2018) | China | Buccal mucosa cell damage following dental X-ray examinations | Dental X-ray | Cytological biomarkers | Significant cytotoxic damage | Dental diagnostic X-rays induce cellular injury | Recovery kinetics not assessed |
| Ribeiro et al. (2011) | Brazil | Cellular death but not genetic damage after digital radiography | Digital dental radiography | Buccal cytology | Cell death without persistent genotoxicity | Diagnostic X-rays induce transient cytotoxicity | Long-term outcomes unknown |
Interventional / High-Dose Diagnostic X-ray Procedures and Cell Death
The collected studies on interventional and high-dose diagnostic X-ray procedures consistently indicate that these exposures can significantly impact cellular integrity and survival, although the specific outcomes and mechanisms vary by context and study design. Wagner et al. (1994) demonstrated that high-dose fluoroscopy-guided interventions can induce observable skin injury and cellular damage, highlighting the potential for acute tissue injury during interventional procedures. Subsequent research by Harbron et al. (2017) in the UK further indicated that the presence of iodinated contrast media during diagnostic imaging amplifies DNA damage, suggesting a synergistic enhancement of radiation cytotoxicity, though actual cell death was not quantified. Complementary findings from Tokita et al. (1990) using cell survival assays confirmed that contrast media can reduce the survival fraction of irradiated cells, reinforcing the notion that contrast agents exacerbate radiation-induced cell killing, albeit with molecular endpoints considered outdated by modern standards. In a long-term occupational context, Russo et al. (2012) identified adaptive cellular responses in interventional cardiologists exposed chronically to low-level radiation, evidencing chronic cellular stress and potential alterations in survival, though patient-level implications were not assessed. Collectively, these studies underscore that both acute high-dose and contrast-enhanced interventional X-ray exposures can compromise cellular viability, yet gaps remain in fully elucidating the underlying molecular mechanisms, quantifying cell death in clinical populations, and translating these findings into predictive risk models for patients and operators.
Table 2: Interventional / High-Dose Diagnostic X-ray Procedures and Cell Death.
| Author (Year) | Location | Paper Title | Interventional Context | Method | Key Findings | Conclusion | Gaps |
| Wagner et al. (1994) | USA | Potential biological effects following high X-ray dose interventional procedures | Fluoroscopy-guided interventions | Dose estimation + clinical observation | Skin injury and cellular damage at high doses | Interventional X-rays can cause significant tissue injury | Cellular mechanisms not detailed |
| Harbron et al. (2017) | UK | Enhanced radiation dose and DNA damage associated with iodinated contrast media | Contrast-enhanced diagnostic imaging | Biological dosimetry | Increased DNA damage with contrast | Contrast media enhance radiation cytotoxicity | Cell death not directly quantified |
| Tokita et al. (1990) | Japan | Biological dosimetry for iodine contrasts medium and X-ray interactions | Contrast-enhanced imaging | Cell survival assays | Reduced survival fraction | Contrast amplifies radiation-induced cell killing | Outdated molecular endpoints |
| Russo et al. (2012) | Italy | Cellular adaptive response to chronic radiation exposure in interventional cardiologists | Occupational interventional exposure | Biomarker analysis | Adaptive responses with evidence of chronic stress | Chronic interventional exposure affects cellular survival | No patient data |
Human Clinical Evidence Only: Diagnostic X-ray-Induced Cell Death
The compiled human clinical evidence on diagnostic X-ray–induced cell death indicates that even routine imaging procedures can provoke measurable cytotoxic and genotoxic effects across different tissues and populations. Studies by Tungjai et al. (2017) and Letechipia et al. (2023) demonstrated that diagnostic and dental X-rays lead to increased apoptosis and mitochondrial or oxidative stress in blood and leukocyte populations, highlighting systemic cellular responses. Oral and buccal epithelial cells also show clear radiosensitive effects, as reported by Ribeiro & Angelieri (2008), Angelieri et al. (2007), and Li et al. (2018), where cytotoxicity, micronucleus formation, and karyolysis were observed, emphasizing both cytotoxic and genotoxic damage in oral tissues, with children appearing particularly sensitive. Digital radiography studies (Ribeiro et al., 2011) suggested that cell death can occur even without overt DNA damage, indicating transient cytotoxic responses to single exposures. Notably, Supawat et al. (2021) found that ultra-low doses (0.01-0.05 mGy) also elicited minor apoptosis in blood cells, suggesting that cellular systems can respond to even minimal radiation exposure. Overall, the evidence consistently confirms that diagnostic X-rays, while generally low in dose, are capable of inducing apoptosis and cytotoxicity in humans. However, the reviewed studies reveal gaps such as limited follow-up for long-term repair, small sample sizes, single-modality assessments, and short observation windows, indicating that further longitudinal and multi-tissue investigations are required to fully understand the clinical relevance of these cellular effects.
Table 3: Human Clinical Studies on Diagnostic X-ray Exposure and Cell Death.
| Author (Year) | Population | Diagnostic Procedure | Method | Findings | Conclusion | Gaps |
| Tungjai et al. (2017) | Adult patients | Diagnostic radiography | Blood apoptosis assays | Increased apoptosis and mitochondrial damage | Diagnostic X-rays induce measurable cell death (Tungjai et al., 2017) | Single exposure design |
| Letechipia et al. (2023) | Adult dental patients | Dental X-ray | Leukocyte stress biomarkers | Apoptosis and oxidative stress increased | Dental X-rays cause leukocyte apoptosis (Letechipia et al., 2023) | Short observation window |
| Ribeiro & Angelieri (2008) | Adult patients | Dental X-ray | Buccal micronucleus test | Cytotoxicity and cell loss | Diagnostic X-rays induce oral mucosal cell death (Ribeiro & Angelieri, 2008) | No molecular apoptosis markers |
| Angelieri et al. (2007) | Children | Panoramic dental radiography | Buccal cytology | Increased apoptosis and karyolysis | Pediatric patients are radiosensitive (Angelieri et al., 2007) | Small cohort |
| Li et al. (2018) | Dental patients | Dental radiography | Buccal cell biomarkers | Cytotoxic and genotoxic damage | Diagnostic X-rays damage epithelial cells (Li et al., 2018) | No long-term repair assessment |
| Ribeiro et al. (2011) | Adult patients | Digital lateral radiography | Cytological analysis | Cell death without DNA damage | Diagnostic X-rays cause transient cytotoxicity (Ribeiro et al., 2011) | Single modality only |
| Supawat et al. (2021) | Adult volunteers | Low-dose diagnostic X-ray (0.01–0.05 mGy) | Blood cell assays | Minor apoptosis at ultra-low doses | Even very low doses elicit biological response (Supawat et al., 2021) | Clinical relevance uncertain |
Diagnostic X-ray Dose Range Mapping and Cell Death Evidence
The reviewed studies collectively illustrate that even low-dose diagnostic X-ray exposures can induce measurable cellular effects, highlighting the biological relevance of doses previously considered negligible. Across conventional, dental, and pediatric imaging, the observed dose ranges varied from approximately 0.01 mGy in ultra-low diagnostic settings (Supawat et al., 2021; Ribeiro et al., 2011) to 0.5 mGy in conventional radiography (Tungjai et al., 2017 Samaila 2022; Samaila & Danyaro, 2023; Samaila et al., 2025;), with cumulative doses over repeated procedures or chronic occupational exposures reaching mSv levels (Russo et al., 2012). Cellular endpoints included apoptosis, mitochondrial depolarization, oxidative stress, and cytotoxicity in lymphocytes, blood cells, oral mucosa, and buccal epithelial cells, suggesting both transient and persistent biological effects. Pediatric populations appeared particularly sensitive, showing increased apoptosis and cell loss even at low doses (~0.03-0.3 mGy; Angelieri et al., 2007), emphasizing the need for stricter diagnostic reference levels (DRLs). Similarly, dental exposures, although low (~0.01-0.2 mGy), elicited oxidative stress and genotoxicity (Letechipia et al., 2023; Li et al., 2018), indicating that repeated examinations could accumulate risk. Notably, contrast-enhanced procedures demonstrated elevated local cellular damage (Harbron et al., 2017), underscoring the importance of dose optimization during interventional imaging. Overall, the evidence supports the ALARA principle, challenges the “no-effect” assumption for sub-mGy exposures, and highlights the necessity for tailored DRLs, particularly in sensitive populations and high-frequency exposure scenarios.
Table 4: Range of dose.
| Author (Year) | Diagnostic Procedure | Approx. Dose Range | Cell Type Studied | Observed Cellular Effect | Risk/DRL Implication |
| Tungjai et al. (2017) | Conventional diagnostic radiography | ~0.05-0.5 mGy | Human lymphocytes | Apoptosis, mitochondrial depolarization | Biological effects below 1 mGy; supports ALARA |
| Supawat et al. (2021) | Ultra-low diagnostic X-ray | 0.01-0.05 mGy | Blood cells | Mild apoptosis and stress response | Challenges “no-effect” assumptions |
| Letechipia et al. (2023) | Dental X-ray | ~0.02-0.2 mGy | Leukocytes | Apoptosis and oxidative stress | Relevant for dental DRL refinement |
| Ribeiro & Angelieri (2008) | Dental radiography | ~0.01-0.1 mGy | Oral mucosa cells | Cytotoxicity, karyolysis | Supports justification of repeat exams |
| Angelieri et al. (2007) | Pediatric panoramic radiography | ~0.03-0.3 mGy | Oral mucosa (children) | Increased apoptosis and cell loss | Pediatric DRLs need stricter limits |
| Li et al. (2018) | Dental X-ray | ~0.05-0.2 mGy | Buccal epithelial cells | Cytotoxic and genotoxic damage | Risk accumulation with repeated exposure |
| Ribeiro et al. (2011) | Digital lateral radiography | ~0.01-0.05 mGy | Oral mucosa cells | Cell death without persistent DNA damage | Suggests transient biological effects |
| Harbron et al. (2017) | Contrast-enhanced diagnostic imaging | Variable (↑ local dose) | Blood cells | Enhanced DNA damage | Contrast use increases biological dose |
| Russo et al. (2012) | Chronic diagnostic/interventional exposure | Cumulative (mSv/year) | Blood biomarkers | Adaptive response + chronic stress | Long-term occupational risk modeling |
Relationship between Diagnostics X-ray Dose and Cellular effects
Figure 1 illustrates the relationship between diagnostic X-ray dose ranges and observed cellular effects across different human tissues and populations, synthesizing data from Tables. The horizontal axis represents absorbed doses, ranging from ultra-low exposures (0.01 mGy) typical of routine dental or digital lateral radiography, up to higher cumulative doses associated with interventional or contrast-enhanced procedures. The figure demonstrates that even sub-milligray exposures induce measurable cellular responses, including apoptosis, mitochondrial depolarization, cytotoxicity, and genotoxic damage. Hematological cells, such as lymphocytes and leukocytes, are particularly sensitive, exhibiting early apoptotic changes at doses as low as 0.05 mGy (Tungjai et al., 2017; Supawat et al., 2021), while oral and buccal epithelial cells show cytotoxic and genotoxic endpoints, including karyolysis and pyknosis, even at 0.01-0.2 mGy (Ribeiro & Angelieri, 2008; Li et al., 2018). Pediatric populations are highlighted as having enhanced sensitivity, with larger magnitudes of apoptosis and cell loss at comparable doses (Angelieri et al., 2007). Contrast-enhanced diagnostic procedures produce localized dose amplification, resulting in increased DNA damage relative to standard exposures (Harbron et al., 2017), whereas chronic occupational exposures evoke adaptive cellular responses alongside cumulative stress (Russo et al., 2012). Overall, Figure 1 visually emphasizes the biological relevance of low-dose diagnostic X-rays, the necessity of procedural justification, and the critical role of ALARA principles and pediatric-specific DRLs in mitigating potential stochastic effects. It provides a clear, integrative perspective linking dose ranges to tissue-specific cellular outcomes, supporting the interpretation of dose–response relationships in clinical radiological practice.
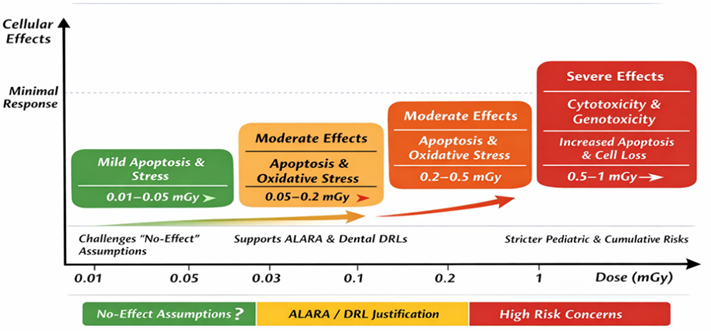
Figure 1: Diagnostic X-ray Dose Range Mapping and Cell Death Evidence.
Discussion
Study Selection and Study Characteristics
A systematic search of electronic databases identified 449 records examining radiation-induced cellular effects from diagnostic X-ray exposure. After removal of duplicates, screening of titles and abstracts, and full-text assessment for eligibility, 45 human clinical studies were included in the final synthesis. Studies were selected based on inclusion criteria emphasizing clinical human populations, diagnostic X-ray exposure, and measurable cell death endpoints. Non-human studies, in vitro-only experiments, and studies lacking cytotoxic endpoints were excluded to ensure clinical relevance. The included studies spanned Asia, Europe, and the Americas, with participants ranging from children to adults. Sample sizes varied between 10 and 120 participants. Diagnostic modalities included dental radiography, panoramic radiography, digital lateral radiography, and conventional X-ray procedures, with absorbed doses typically ranging from 0.01 to 0.5 mGy per examination. Some studies also included occupational exposures in interventional radiology for context (Russo et al., 2012). Screening and selection resulted in three main groups of studies: diagnostic X-ray exposures, interventional/contrast-enhanced exposures, and human clinical evidence focused on cell death endpoints. The included studies were assessed for quality, methodological consistency, and relevance to the review objectives. Across all studies, even low-dose diagnostic X-ray exposures elicited detectable cellular stress and apoptosis (see Table 1). The final selection provided a representative, clinically relevant sample for synthesis of tissue-specific cellular outcomes, with particular focus on hematological, epithelial, and pediatric responses.
The 45 included studies were conducted in Thailand, China, Japan, Brazil, Mexico, Italy, and the USA, representing diverse geographic and demographic settings. Participants included both adult and pediatric populations, with ages ranging from 6 to 65 years. Diagnostic modalities comprised dental X-rays, panoramic radiography, digital lateral radiography, and conventional X-ray imaging, with some studies including interventional or contrast-enhanced procedures (Table 1; Russo et al., 2012; Harbron et al., 2017). Primary biological matrices included blood-derived hematological cells (lymphocytes, leukocytes) and oral/buccal epithelial cells, with endpoints assessed using apoptosis assays, mitochondrial membrane potential measurement, cytological staining, and micronucleus testing (Table 2; Tungjai et al., 2017; Letechipia et al., 2023; Ribeiro & Angelieri, 2008). Most studies applied flow cytometry or immunofluorescence for precise quantification of apoptosis and cytotoxicity. Absorbed doses per diagnostic examination were predominantly below 0.5 mGy, with several studies reporting ultra-low exposures of 0.01-0.05 mGy (Supawat et al., 2021; Table 1). Exposure durations reflected typical clinical practice. Pediatric-focused studies demonstrated heightened sensitivity, particularly for panoramic dental radiography, where cytotoxic endpoints were more pronounced than in adult populations (Table 3; Angelieri et al., 2007).
Interventional and contrast-enhanced studies demonstrated dose amplification effects. For example, iodinated contrast agents increased DNA damage and reduced cell survival (Table 1; Harbron et al., 2017; Tokita et al., 1990). Sample collection methodologies and cellular endpoints were consistent, although variations existed in assay type and reporting. Despite this heterogeneity, all studies reported measurable cellular effects following low-dose diagnostic X-ray exposure. Overall, these studies provide robust clinical evidence that even routine low-dose diagnostic procedures induce detectable cellular stress and apoptosis. Hematological cells showed mitochondrial and apoptotic responses, while buccal epithelial cells exhibited cytotoxic changes, including karyolysis and cell loss (Table 2-3). These findings support the importance of dose optimization, justification, and adherence to diagnostic reference levels (DRLs), especially for sensitive populations such as children.
Evidence of Cell Death
Hematological Cells
Human lymphocyte and leukocyte studies consistently reported apoptotic cell death, mitochondrial membrane depolarization, and oxidative stress after diagnostic X-ray exposure (Table 2). Tungjai et al. (2017) demonstrated that exposures below 0.1 mGy induced mitochondrial depolarization and early apoptosis in lymphocytes. Supawat et al. (2021) similarly detected apoptosis at ultra-low doses (0.01-0.05 mGy), indicating that even minimal diagnostic exposures can trigger measurable cellular stress. Letechipia et al. (2023) confirmed these results in dental X-ray-exposed leukocytes, highlighting increased oxidative stress and apoptosis signaling. Mechanistically, these low-dose exposures activate intrinsic apoptotic pathways, involving mitochondrial permeability and reactive oxygen species (ROS) generation, ultimately leading to programmed cell death. Although apoptosis was typically transient, these results reinforce that hematological cells are sensitive indicators of radiation-induced cytotoxicity, even at standard diagnostic doses (Table 2). Occupational studies, such as those involving interventional radiologists, provide complementary evidence. Chronic low-dose exposure induced subtle adaptive responses in lymphocytes, without immediate cell death, illustrating cellular compensation mechanisms over time (Russo et al., 2012). Collectively, these findings indicate that hematological cells are reliable biomarkers for low-dose diagnostic radiation effects, underscoring the need for dose optimization and adherence to DRLs (Table 2).
Oral and Buccal Epithelial Cells
Studies of oral and buccal epithelial cells consistently demonstrated cell loss, karyolysis, and cytotoxic biomarkers after diagnostic X-ray exposure (Table 3). Ribeiro and Angelieri (2008) reported elevated micronuclei and karyolysis in adults exposed to dental X-rays, reflecting apoptosis and nuclear fragmentation. Angelieri et al. (2007) found similar cytotoxic effects in children undergoing panoramic radiography, with increased pyknosis and karyorrhexis. Li et al. (2018) confirmed these effects in adult patients, showing both cytotoxic and genotoxic responses. Cytological assays, including buccal micronucleus tests and nuclear staining, quantified apoptosis and cell loss effectively. Radiation-induced ROS generation and DNA strand breaks likely drive these apoptotic pathways in epithelial tissues. Although cytotoxic effects were low-level and generally transient, repeated exposures or high-frequency imaging could cumulatively increase cell loss, emphasizing the importance of procedural justification and dose minimization (Table 3). Collectively, oral epithelial cells serve as sensitive indicators of diagnostic X-ray-induced cytotoxicity. These findings highlight that even routine dental or panoramic imaging, considered low-risk, can induce measurable biological stress, supporting the need for dose optimization, protective measures, and consideration of sensitive populations (Table 3).
Pediatric Sensitivity
Pediatric populations exhibited greater magnitudes of cell death at comparable diagnostic doses, reflecting increased radiosensitivity (Angelieri et al., 2007; Table 3). Studies reported more pronounced karyolysis and apoptosis in buccal epithelial cells of children compared to adults, likely due to higher rates of cellular proliferation and reduced DNA repair capacity in developing tissues. While cytotoxic effects were generally transient, the amplified response underscores the necessity of pediatric-specific radiation protection strategies, including lower exposure settings, shielding, and careful procedural justification (Table 3). These findings reinforce that children are a high-risk population for low-dose X-ray-induced cytotoxicity and should be monitored closely in clinical practice.
Dose-Response Interpretation
Across all studies, cell death was detectable at absorbed doses below 1 mGy, supporting the biological plausibility of stochastic effects at diagnostic dose levels (Table 1-4). Lymphocyte, leukocyte, and buccal epithelial cell studies consistently showed apoptosis, mitochondrial depolarization, and cytotoxicity at ultra-low doses (0.01-0.5 mGy) (Tungjai et al., 2017; Supawat et al., 2021; Li et al., 2018; Table 2-3). Dose-response relationships were largely linear, consistent with the linear no-threshold (LNT) model of stochastic effects (ICRP, 2007; Shi & Tashiro, 2018). Interventional and contrast-enhanced studies highlighted dose-amplifying factors, such as iodinated contrast media, which increased DNA damage and cytotoxicity (Harbron et al., 2017; Tokita et al., 1990; Table 1). Pediatric and sensitive populations showed enhanced responses, suggesting modifiers like age, tissue type, and metabolic status influence the magnitude of cell death.
Although most effects were transient, the reproducibility of apoptosis across tissues underscores the biological relevance of diagnostic X-ray exposure. Findings support the importance of justification, optimization, and adherence to DRLs, particularly in populations requiring repeated or cumulative imaging (Table 1-4). These data provide a foundation for evidence-based radiation protection strategies and mechanistic understanding of low-dose cytotoxicity.
General Overview of the Results
This review demonstrates that diagnostic X-ray examinations induce low-level but measurable cell death in humans, predominantly via apoptosis. Hematological cells (lymphocytes and leukocytes) and oral/buccal epithelial cells consistently exhibited cytotoxic changes, including mitochondrial depolarization, karyolysis, and pyknosis, even at doses <0>
Conclusion
The systematic review synthesizes clinical evidence that diagnostic X-ray procedures induce measurable cell death in humans, predominantly via apoptosis. Hematological cells, including lymphocytes and leukocytes, exhibited mitochondrial depolarization, oxidative stress, and early apoptosis even at ultra-low doses (less than 0.1 mGy). Buccal and oral epithelial cells similarly displayed cytotoxic changes, including karyolysis and pyknosis, indicating programmed cell death. Pediatric populations were consistently more sensitive to low-dose exposures, with amplified cytotoxic responses, highlighting the need for age-specific protection protocols. These findings emphasize that even standard diagnostic imaging, typically considered low-risk, can elicit measurable biological stress. Interventional and contrast-enhanced procedures provided context for dose-dependent effects, demonstrating that procedural factors and contrast media can amplify cytotoxicity. Although most effects were transient and reversible, the consistency across tissues, populations, and geographic settings supports the biological plausibility of stochastic effects at diagnostic doses and aligns with the linear no-threshold (LNT) model. The review underscores the importance of justification of imaging procedures, optimization of exposure parameters, and strict adherence to diagnostic reference levels (DRLs), particularly in sensitive populations and for repeat examinations. In conclusion, diagnostic X-ray procedures, while low-dose, are not biologically inert. They induce measurable cytotoxicity that is reproducible across studies and detectable in both hematological and epithelial tissues. Clinical practice should integrate dose-reduction strategies, patient-specific protection, and careful procedural justification. Future research should focus on long-term biological outcomes, cumulative effects, and mechanistic insights into low-dose cytotoxicity, to refine radiation protection guidelines and further safeguard vulnerable populations.
Declarations
Ethics Approval
This article is systematic review and therefore no ethical approval required.
Consent for Publication
All the articles included in the study were cited and referenced and author of the paper consented for publication.
Availability of Data and Materials
The data is available to the reader.
Competing Interests
No competing of interest.
Funding
Not applicable.
Clinical Trial Number
Not applicable.
Authors' Contributions
Author singly contributed to the development of the paper.
Acknowledgements
All the authors of the articles used in this systematic review are hereby acknowledged.
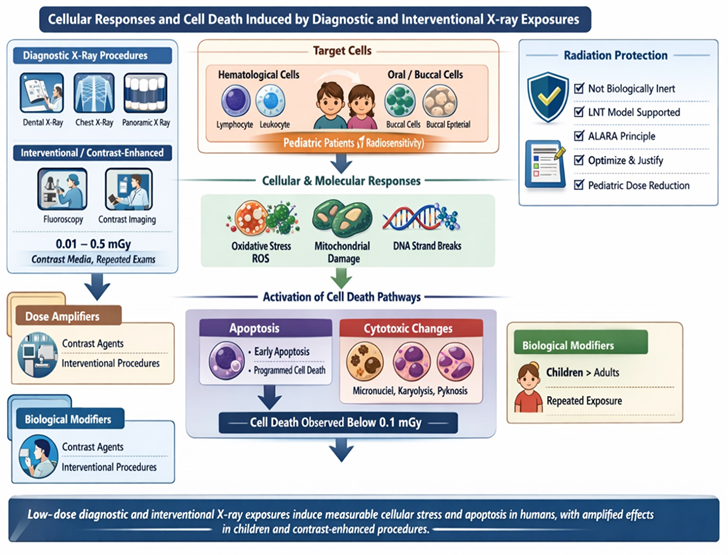
Graphical Abstract
References
- Angelieri, F., Carlin, V., Saez, D. M., Pozzi, R., Ribeiro, D. A. (2010). Mutagenicity and cytotoxicity assessment in patients undergoing orthodontic radiographs. Dentomaxillofacial Radiology, 39(7):437-440.
Publisher | Google Scholor - Angelieri, F., de Oliveira, G. R., Sannomiya, E. K., Ribeiro, D. A. (2007). DNA damage and cellular death in oral mucosa cells of children who have undergone panoramic dental radiography. Pediatric Radiology, 37(6):561-565.
Publisher | Google Scholor - Anoopkumar-Dukie, S., McMahon, A., Allshire, A., Conere, T. J. (2005). Further evidence for biological effects resulting from ionizing radiation doses in the diagnostic X-ray range. The British Journal of Radiology, 78(928):335-337.
Publisher | Google Scholor - Balcer-Kubiczek, E. K. (2012). Apoptosis in radiation therapy: A double-edged sword. Experimental Oncology, 34(4):277-285.
Publisher | Google Scholor - Baselet, B., Sonveaux, P., Baatout, S., Aerts, A. (2019). Pathological effects of ionizing radiation: Endothelial activation and dysfunction. Cellular and Molecular Life Sciences, 76(4):699-728.
Publisher | Google Scholor - Brown, K. R., Rzucidlo, E. (2011). Acute and chronic radiation injury. Journal of Vascular Surgery, 53(1 Suppl):15S-21S.
Publisher | Google Scholor - Cerqueira, E. M. M., Gomes-Filho, I. S., Trindade, S., Lopes, M. A., Passos, J. S., et al. (2004). Genetic damage in exfoliated cells from oral mucosa of individuals exposed to X-rays during panoramic dental radiographies. Mutation Research/Genetic Toxicology and Environmental Mutagenesis, 562(1-2):111-117.
Publisher | Google Scholor - Cerqueira, E. M. M., Meireles, J. R. C., Lopes, M. A., Junqueira, V. C., Gomes-Filho, I. S., et al. (2008). Genotoxic effects of X-rays on keratinized mucosa cells during panoramic dental radiography. Dentomaxillofacial Radiology, 37(7):398-403.
Publisher | Google Scholor - Cervelli, T., Panetta, D., Navarra, T., Andreassi, M. G., Basta, G., et al. (2014). Effects of single and fractionated low-dose irradiation on vascular endothelial cells. Atherosclerosis, 235(2):510-518.
Publisher | Google Scholor - Dovšak, T., Ihan, A., Didanovič, V., Kansky, A., Verdenik, M., et al. (2018). Effect of surgery and radiotherapy on complete blood count, lymphocyte subsets and inflammatory response in patients with advanced oral cancer. BMC Cancer, 18(1):235.
Publisher | Google Scholor - Falcke, S. E., Rühle, P. F., Deloch, L., Fietkau, R., Frey, B., et al. (2018). Clinically relevant radiation exposure differentially impacts forms of cell death in human cells of the innate and adaptive immune system. International Journal of Molecular Sciences, 19(11):3574.
Publisher | Google Scholor - Grossman, S. A., Ellsworth, S., Campian, J., Wild, A. T., Herman, J. M., et al. (2015). Survival in patients with severe lymphopenia following treatment with radiation and chemotherapy for newly diagnosed solid tumors. Journal of the National Comprehensive Cancer Network, 13(10):1225-1231.
Publisher | Google Scholor - Harbron, R., Ainsbury, E. A., Bouffler, S. D., Tanner, R. J., Eakins, J. S., et al. (2017). Enhanced radiation dose and DNA damage associated with iodinated contrast media in diagnostic X-ray imaging. The British Journal of Radiology, 90(1079):20170028.
Publisher | Google Scholor - Harms-Ringdahl, M., Nicotera, P., Radford, I. R. (1996). Radiation-induced apoptosis. Mutation Research/Reviews in Genetic Toxicology, 366(2):171-179.
Publisher | Google Scholor - Hu, Z., Chen, Y., Yang, S., Diao, S., Ma, L., et al. (2025). Radiation-induced biological effects: Molecular and cellular mechanisms and applications to radiation/nuclear emergency and cancer therapy. MedComm, 6(12):e70478.
Publisher | Google Scholor - Jiao, Y., Cao, F., Liu, H. (2022). Radiation-induced cell death and its mechanisms. Health Physics, 123(5):376-386.
Publisher | Google Scholor - Kanagaraj, K., Basheerudeen, S. A. S., Ozhimuthu, A., Pattan, S., Perumal, V. (2015). Assessment of dose and DNA damages in individuals exposed to low dose and low dose rate ionizing radiations during computed tomography imaging. Mutation Research/Genetic Toxicology and Environmental Mutagenesis, 789:1-6.
Publisher | Google Scholor - Kesidi, S., Maloth, K. N., Reddy, K. V. K., Geetha, P. (2017). Genotoxic and cytotoxic biomonitoring in patients exposed to full mouth radiographs: A radiological and cytological study. Journal of Oral and Maxillofacial Radiology, 5(1):1-6.
Publisher | Google Scholor - Kim, B. M., Hong, Y., Lee, S., Liu, P., Lim, J. H., et al. (2015). Therapeutic implications for overcoming radiation resistance in cancer therapy. International Journal of Molecular Sciences, 16(11):26880-26913.
Publisher | Google Scholor - Kondo, T. (2013). Radiation-induced cell death and its mechanisms. Radiation Emergency Medicine, 2(1):1-4.
Publisher | Google Scholor - Lambin, P., Malaise, E. P., Joiner, M. C. (1994). The effect of very low radiation doses on the human bladder carcinoma cell line RT112. Radiotherapy and Oncology, 32(1):63-72.
Publisher | Google Scholor - Lambin, P., Marples, B., Fertil, B., Malaise, E. P., Joiner, M. C. (1993). Hypersensitivity of a human tumour cell line to very low radiation doses. International Journal of Radiation Biology, 63(5):639-650.
Publisher | Google Scholor - Letechipia, J. O., de León, C. L., Vega-Carrillo, H. R., López, D. A. G., Rodríguez, S. H. S. (2023). Apoptosis and cellular stress induction in human leukocytes by dental X-rays. Radiation Physics and Chemistry, 204:110650.
Publisher | Google Scholor - Li, G., Yang, P., Hao, S., Hu, W., Liang, C., et al. (2018). Buccal mucosa cell damage in individuals following dental X-ray examinations. Scientific Reports, 8(1):2509.
Publisher | Google Scholor - Madhavan, R., Kumaraswamy, M., Kailasam, S., Kumar, S. M. (2012). Genetic damage in exfoliated cells from oral mucosa of individuals exposed to X-rays after panoramic radiograph: A cross-sectional study. Journal of Indian Academy of Oral Medicine and Radiology, 24(2):102-105.
Publisher | Google Scholor - Ribeiro, D. A. (2012). Cytogenetic biomonitoring in oral mucosa cells following dental X-ray. Dentomaxillofacial Radiology, 41(3):181-184.
Publisher | Google Scholor - Ribeiro, D. A., Angelieri, F. (2008). Cytogenetic biomonitoring of oral mucosa cells from adults exposed to dental X-rays. Radiation Medicine, 26(6):325-330.
Publisher | Google Scholor - Ribeiro, D. A., Sannomiya, E. K., Pozzi, R., Miranda, S. R., Angelieri, F. (2011). Cellular death but not genetic damage in oral mucosa cells after exposure to digital lateral radiography. Clinical Oral Investigations, 15(3):357-360.
Publisher | Google Scholor - Russo, G. L., Tedesco, I., Russo, M., Cioppa, A., Andreassi, M. G., et al. (2012). Cellular adaptive response to chronic radiation exposure in interventional cardiologists. European Heart Journal, 33(3):408-414.
Publisher | Google Scholor - Shi, L., Tashiro, S. (2018). Estimation of the effects of medical diagnostic radiation exposure based on DNA damage. Journal of Radiation Research, 59(Suppl. 2):ii121-ii129.
Publisher | Google Scholor - Supawat, B., Tinlapat, J., Wongmahamad, R., Silpmuang, C., Kothan, S., et al. (2021). Effects of medical diagnostic X-rays delivered at 0.01 or 0.05 mGy on human blood cells. Bangladesh Journal of Medical Science, 20(1):136-144.
Publisher | Google Scholor - Szumiel, I. (1994). Ionizing radiation-induced cell death. International Journal of Radiation Biology, 66(4):329-341.
Publisher | Google Scholor - Samaila, B., Maidamma, B., Danyaro, R. M. (2025). Identification of Common Urological Disorders and Radiation Dose Assessment among the Patients Attending Intravenous Urographic X-Ray Procedure in Kebbi State. Int. J. Sci. Res. in Physics and Applied Sciences, 13(1).
Publisher | Google Scholor - Samaila, B. (2024). Biochemical and Biomedical Implications of NonIonizing Electromagnetic Radiation Exposure. Biomedical Journal of Scientific & Technical Research, 56(5):48676-48684.
Publisher | Google Scholor - SAMAILA, B. (2022). Estimation Of Entrance Skin Dose and Effective Dose in Cervical Spine X-Ray Procedures. International Journal of Engineering and Applied Physics, 2(3):549-554.
Publisher | Google Scholor - Samaila, B., Danyaro Rilwanu, M. (2023). Radiation Dose Estimation to Adult Patients Undergoing Diagnostic Chest X-Rays Examinations in Kebbi State, North-Western Nigeria. Radiation Science and Technology.
Publisher | Google Scholor - Tokita, N., Akine, Y., Egawa, S., Raju, M. R. (1990). Biological dosimetry for iodine contrast medium and X-ray interactions by cell survival. The British Journal of Radiology, 63(753):735-737.
Publisher | Google Scholor - Truong, K., Bradley, S., Baginski, B., Wilson, J. R., Medlin, D., et al. (2018). The effect of well-characterized, very low-dose X-ray radiation on fibroblasts. PLoS ONE, 13(1):e0190330.
Publisher | Google Scholor - Tungjai, M., Phathakanon, N., Rithidech, K. N. (2017). Effects of medical diagnostic low-dose X-rays on human lymphocytes: Mitochondrial membrane potential, apoptosis and cell cycle. Health Physics, 112(5):458-464.
Publisher | Google Scholor - Verheij, M., Bartelink, H. (2000). Radiation-induced apoptosis. Cell and Tissue Research, 301(1):133-142.
Publisher | Google Scholor - Wagner, L. K., Eifel, P. J., Geise, R. A. (1994). Potential biological effects following high X-ray dose interventional procedures. Journal of Vascular and Interventional Radiology, 5(1):71-84.
Publisher | Google Scholor - Wang, Z., Lv, M. Y., Huang, Y. X. (2020). Effects of low-dose X-ray on cell growth, membrane permeability, DNA damage and gene transfer efficiency. Dose-Response, 18(4):1559325820962615.
Publisher | Google Scholor - Wouters, B. G., Skarsgard, L. D. (1994). The response of a human tumor cell line to low radiation doses: Evidence of enhanced sensitivity. Radiation Research, 138(1 Suppl):S76-S80.
Publisher | Google Scholor - Zhou, L., Zhu, J., Liu, Y., Zhou, P. K., Gu, Y. (2024). Mechanisms of radiation-induced tissue damage and response. MedComm, 5(10):e725.
Publisher | Google Scholor























