

Case Report
Beyond the Facade: A Case of Cardiac Amyloidosis Featuring Aberrant Papillary Muscle Insertion Resembling Hypertrophic Obstructive Cardiomyopathy
- A.El haidoudi *
- M.Ouacha
- E.massri
- N.Lahmouch
- N. Doghmi
- R. Amri
- M. Cherti
Department of cardiology B – Ibn sina university hospital center, Rabat, Morocco.
*Corresponding Author: A.El haidoudi, Department of cardiology B – Ibn sina university hospital center, Rabat, Morocco.
Citation: A.El haidoudi, Ouacha M., E.massri, Lahmouch N., Doghmi N., Amri R. et al. (2026). Beyond the Facade: A Case of Cardiac Amyloidosis Featuring Aberrant Papillary Muscle Insertion Resembling hypertrophic obstructive cardiomyopathy, Academic Journal of Clinical Research and Reports, BioRes Scientia Publishers. 2(1):1-3. DOI: 10.59657/3067-0438.brs.26.040
Copyright: © 2026 A.El haidoudi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 23, 2026 | Accepted: April 20, 2026 | Published: May 01, 2026
Abstract
Anomalous insertion of the papillary muscle (PM) or chordae tendineae constitutes a rare yet clinically significant factor contributing to dynamic left ventricular outflow tract (LVOT) obstruction in individuals diagnosed with hypertrophic cardiomyopathy or cardiac amyloidosis. These anomalies pose a diagnostic challenge, particularly with 2-dimensional echocardiography (2-DEcho), and accurate identification is paramount in determining the appropriateness of an extended septal myectomy over a standard procedure for symptom relief.
Keywords: cardiac amyloidosis; papillary muscle insertion; hypertrophic; cardiomyopathy
Introduction
Anomalous insertion of the papillary muscle (PM) or chordae tendineae constitutes a rare yet clinically significant factor contributing to dynamic left ventricular outflow tract (LVOT) obstruction in individuals diagnosed with hypertrophic cardiomyopathy or cardiac amyloidosis. These anomalies pose a diagnostic challenge, particularly with 2-dimensional echocardiography (2-DEcho), and accurate identification is paramount in determining the appropriateness of an extended septal myectomy over a standard procedure for symptom relief.
We present the case of a 74-year-old woman with an anomalous papillary muscle insertion and amyloidosis, initially misinterpreted as obstructive hypertrophic cardiomyopathy. The case underscores the complexity and importance of precise diagnostic differentiation in guiding appropriate therapeutic interventions, such as considering an extended septal myectomy
Case Presentation
We present the case of a 74-year-old woman devoid of cardiovascular risk factors. She reported Stage II dyspnea persisting for the past 7 years, leading to her initial consultation 5 years ago. At that time, hypertrophic cardiomyopathy with systolic anterior motion was diagnosed, and the patient was commenced on beta-blocker therapy.
Over the subsequent years, there was a gradual decline in her condition, accompanied by the progressive onset of lower limb edema, prompting her recent consultation with our department.
Upon admission, physical examination revealed a maximal systolic murmur at the aortic focus, which diminished in severity during Valsalva maneuver. Tricuspid insufficiency murmur, signs indicative of right heart failure, and an exaggerated pulmonary second sound were also noted.
Electrocardiography indicated atrial fibrillation with left ventricular hypertrophy, while transthoracic echocardiography disclosed an 18-mm homogenous left ventricular hypertrophy featuring a bifid, low-inserted lateral papillary muscle directly attaching to the anterior mitral leaflet. This structural anomaly contributed to left ventricular outflow tract obstruction, with a maximal gradient of 96 mmHg, which also exhibited reduction with Valsalva maneuver. Additionally, severe tricuspid insufficiency and a high likelihood of pulmonary hypertension were observed. Subsequent magnetic resonance imaging supported the suspicion of cardiac amyloidosis, a diagnosis later confirmed by nuclear imaging as transthyretin amyloidosis.
Discussion
We present a case of cardiac amyloidosis characterized by an anomalous insertion of the papillary muscle, resulting in left ventricular outflow tract (LVOT) obstruction. While dynamic LVOT obstruction is documented in cardiac amyloidosis, the association with anomalous papillary muscle (PM) insertion has not been previously reported [1]. Two-dimensional echocardiography identified a thickened PM in the context of amyloidosis.
The etiology of dynamic LVOT obstruction is intricate and lacks a precise definition. We postulate that amyloid infiltration may contribute to the anomalous PM's role in this obstruction, influencing hemodynamic and muscle mechanics alongside anomalous PM insertion and mitral leaflet stiffening. In response to amyl nitrate provocation, our case exhibited obstruction closer to the rigid anomalous PM insertion, characterized by non-systolic anterior motion (SAM), indicative of PM thickening due to amyloid infiltration rather than contractile muscle cells [2].
Despite the generally unfavorable prognosis in severe cardiac amyloidosis, reported cases describe attempts to alleviate dynamic LVOT obstruction, including coronary artery bypass grafting with septal myectomy or isolated percutaneous transluminal septal myocardial ablation. Recognizing the presence of anomalous PM is crucial, as mere resolution of thickened septal muscle may not effectively mitigate the pressure gradient.
The diagnosis of anomalous PM leading to dynamic LVOT obstruction poses challenges with 2-D echocardiography. The oblique course of the PM necessitates multiple off-axis images and is time-consuming for comprehensive delineation. Comparative analysis of 2-D echocardiograms in an optimal plane, demonstrating flow acceleration and aliasing in the LVOT, may unveil anatomical discontinuity between the mitral annulus base and the LV walls.
In cases involving mid-cavity obstruction, originating from the anomalous PM or chordae tendineae directly inserted into the mitral valve base, a more extensive myectomy is imperative. This involves a combination of standard operation with extended midventricular resection and additional resection around the bases of the PM. Complete division of all areas of PM fusion to the septum or ventricular walls, along with the division or excision of anomalous chordal structures and fibrous attachments of the mitral leaflets to the ventricular septum or free wall, is essential for optimal management [3].
Continuous-wave Doppler (CW Doppler) demonstrating left ventricular outflow tract (LVOT) obstruction.
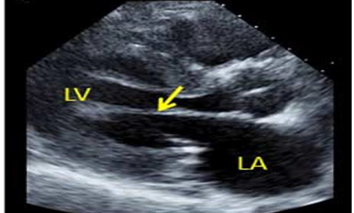
Figure 1: Anomalies in the insertion of the mitral valve apparatus play a contributory role in left ventricular outflow tract (LVOT) obstruction.
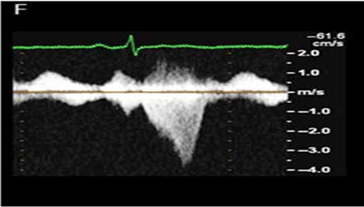
Figure 2: Continuous-wave Doppler (CW Doppler) demonstrating left ventricular outflow tract (LVOT) obstruction.
References
- Klues, H. G., Maron, B. J., Dollar, A. L., & Roberts, W. C. (1992). Diversity of structural mitral valve alterations in hypertrophic cardiomyopathy. Circulation, 85(5):1651–1660.
Publisher | Google Scholor - Klues, H. G., Roberts, W. C., & Maron, B. J. (1991). Anomalous insertion of papillary muscle directly into anterior mitral leaflet in hypertrophic cardiomyopathy: Significance in producing left ventricular outflow obstruction. Circulation, 84(3):1188–1197.
Publisher | Google Scholor - Murphy, R. T., Ratliff, N. B., Lever, H. M., & Kapadia, S. R. (2006). Use of percutaneous transluminal septal myocardial ablation for relief of outflow tract obstruction in cardiac amyloidosis: A novel therapeutic target. Catheterization and Cardiovascular Interventions, 68(4):637–641.
Publisher | Google Scholor























