

Research Article
Assessment of Breast Cancer Knowledge and Screening Services Amongst Women of Reproductive Age Group in North Western Nigeria
- Musa Yakubu *
1 Department of community Medicine College of medicine Federal university Gusau, Zamfara State, Nigeria.
2 University Health Services Ahmadu Bello University Zaria Kaduna State, Nigeria.
*Corresponding Author: Musa Yakubu, Department of community Medicine College of medicine Federal university Gusau, Zamfara State, Nigeria.
Citation: Yakubu M, Ojowu M. Yakubu. (2026). Assessment of Breast cancer knowledge and screening services amongst women of reproductive age group in north Western Nigeria, Journal of BioMed Research and Reports, BioRes Scientia Publishers. 10(4):1-8. DOI: 10.59657/2837-4681.brs.26.241
Copyright: © 2026 Musa Yakubu, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 28, 2026 | Accepted: March 16, 2026 | Published: April 06, 2026
Abstract
Breast Cancer is a public health problem in Nigeria with studies reporting low levels of awareness and practice of breast examination (an important method of prevention). In recent times mortality rates associated with breast cancer have increased tremendously, ranking this disease the 5th leading cause of death, as well as the most common cancer among women worldwide. Regardless of resource level, all countries can implement the basic components of cancer control and prevention namely: early detection, diagnosis and treatment, and palliative care – and thus avoid and cure many cancers, as well as palliating the suffering.
The aim of this study is to assess the awareness, knowledge and screening practices of breast cancer among women in military cantonments in Kaduna State, Nigeria.
Keywords: breast cancer; prevention; knowledge awareness
Introduction
Breast cancer (BC) is the leading female malignancy in the world as well as in Nigeria, accounting for 35% of all female cancers and the leading cause of cancer related death in women. It is the commonest cause of death in developed countries in middle aged women [1-6] In 2010, nearly 1.6 million women worldwide were diagnosed with breast cancer, accounting for approximately 25% of all cancer cases and 14% of the cancer deaths in women.5 In 2012, a total of 1.7million new cases of breast cancer were identified across the globe, which represented about 12% of all new cancer cases and 35% of all cancers in women, furthermore, there were 6.3 million women alive who had been diagnosed with breast cancer in the previous five years.7 Although, breast cancer previously thought to be a disease of the developed world but with almost 50-53 percent of all breast cancer cases and 58% of breast cancer deaths in 2012 now occurring in less developed countries, this line of thought has now changed [3,8,9].
Early-stage disease is associated with a better prognosis than late-stage disease [11]. The five-year breast cancer survival rate in Nigeria is less than 10% compared with over 70% in Western Europe and North America, Earlier stage at diagnosis, combined with therapeutic advances, was a major contributor to the sharp reductions in breast cancer mortality rates in the past two decades in most High-Income Countries [12]. By contrast, most patients with breast cancer in sub-Saharan Africa present with late-stage disease, thought to be due to poor awareness, an absence of organised early detection programmes, and poor facilities for accurate and timely diagnosis and treatment [13-20]. This lapse of time between awareness of a problem and seeking medical attention can affect diagnosis, treatment and prognosis.
Women need to be ‘breast aware’. By being ‘breast aware’, a woman is able to recognise symptoms of breast cancer through regular breast examination practice.
It is in line with this awareness campaign that the WHO chose the 5th day of October every year as a day set aside to raise awareness on breast cancer in order to increase advocacy and support for breast cancer detection and early management of the disease.
Materials and Methods
Study Area
There are three military cantonments in Kaduna State namely Ribadu Military Cantonment, Jaji Military Cantonment and Depot Nigerian Army (Depot NA). The 4 Demonstration battalion is located in Jaji Military Cantonment (45 km from Zaria on the Kano-Kaduna high way).
The Medical centre in the cantonments offer medical services such as out-patient consultation, family health services, routine immunization services, Health Education, prenatal, antenatal and post-natal services, laboratory services, special disease clinics (TB, HIV), Pharmaceutical services, environmental health services, and referral to tertiary health centres, the medical director (usually a military officer) serves as the medical adviser to the commandant.
Study Design
Cross-sectional descriptive mixed method study involving 303 women of reproductive age group, randomly selected from military cantonments in Kaduna State.
Study Population
The study population included all women resident in Military Cantonments in Kaduna State.
Inclusion criteria
Any woman within reproductive age group who is a resident of the cantonment for at least six months before the study and shall not be relocating out of any of the cantonments during the period of the study.
Exclusion criteria
Age: If less than 20 years old. (This is because breast examination is recommended from age 20 years).
Sample Size Determination
The formula for populations less than 10,000 as given by Araoye [22] is given as follows:

Where n=minimum sample size for a single population parameter; Z=Normal standard deviation (1.96); P=Proportion of respondence who practice BSE from previous study2; d=desired precision; q=proportion of respondence not practicing BSE; In addition to 10% non-response; n=302
For the qualitative component, fifteen women (minimum sample size required to reach saturation) [21] were purposively selected based on their position in the barrack (hall leaders) in such a way to represent each age category, ethnicity, religion and rank of husband. In-depth interview was conducted with one women leader per block.
Community entry
At the beginning of the study, familiarization and advocacy visits were undertaken to the Commandant’s and women leaders in each of the study arm.
Sampling Technique
For the quantitative component of the study, multistage sampling technique was used to select study participants as enumerated below:
Stage 1 (Selection of study cantonment): One cantonment was selected from the list of three cantonments in Kaduna State, using simple random sampling via a method of balloting.
Stage 2 (Selection of study barrack within the cantonment): There are three barracks within Chindit Military Cantonment, one barrack was selected from the outcome of stage using the method of balloting.
Stage 3 (Selection of study participants): In the selected barrack, the participants were stratified into civilians, soldiers and officers. The sample size was proportionately allocated to each of the stratum based on population size. The allocation is shown in table 1.
Table 1: Female population and sample allocation in study
| Group | Civilian | Soldiers | Officers | Total | ||||
| Total | Sample | Total | Sample | Total | Sample | Total | Sample | |
| Depot NA | 2960 | 285 | 133 | 13 | 36 | 4 | 3129 | 302 |
Results
Table 2: Socio-demographic characteristics of respondence
| Variable(s) | Frequency n=303 | Percentage (%) |
| Age (years) | ||
| <30> | 114 | 37.6 |
| 30-39 | 155 | 51.2 |
| 40-49 | 32 | 10.6 |
| ≥50 | 2 | 0.7 |
| Religion | ||
| Christianity | 190 | 63 |
| Islam | 122 | 40.3 |
| Level of Education | ||
| None | 1 | 0.3 |
| Informal | 7 | 2.3 |
| Primary | 52 | 17.2 |
| Secondary | 226 | 74.6 |
| Tertiary | 17 | 5.6 |
| Marital Status | ||
| Single | 2.4 | 8 |
| Married | 284 | 93.7 |
| Widowed | 11 | 3.6 |
| Ethnicity | ||
| Igbo | 21 | 6.9 |
| Hausa | 159 | 52.5 |
| Yoruba | 55 | 18.2 |
| *Others | 68 | 22.4 |
| Awareness of Breast Cancer | ||
| Yes | 260 | 85.8 |
| No | 43 | 14.2 |
| BSE | ||
| Yes | 170 | 56.1 |
| No | 133 | 43.9 |
| CBE | ||
| Yes | 173 | 57.1 |
| No | 130 | 42.9 |
| Mammography | ||
| Yes | 17 | 5.6 |
| No | 286 | 94.4 |
| knowledge of breast cancer | ||
| Breast cancer is the most common cancer among Nigerian women | 98 | 32.3 |
| Breast cancer usually presents as a painless breast lump | 75 | 24.8 |
| Early diagnosis improves outcome of treatment | 185 | 61.1 |
| Breast self-examination is useful in early diagnosis | 164 | 54.1 |
| Change in the colour or shape of the breast may be a sign of BC | 132 | 43.6 |
| Right person to carry out BSE | 87 | 28.7 |
| Right person to carry out CBE | 95 | 31.4 |
| Right person to carry out mammography | 25 | 8.3 |
| Frequency of Breast Self-examination | 116 | 38.3 |
| Frequency of Clinical Breast Examination | 33 | 10.9 |
| Frequency of mammography | 3 | 1.0 |
The age ranged 20 to 54 years with a mean age of 32.3 (±6.6years) with majority of the participants being Christians (63%), furthermore, 74.6% of the respondence had secondary level education as their highest educational attainment. The level of awareness of BC, BSE and CBE was 260 (85.8%),170(56.1%) and 173(57.1%) respectively. While awareness of Mammography was 17(5.6%), furthermore 164(54.1%) know that BSE is useful in early diagnosis, as shown in Table 2.
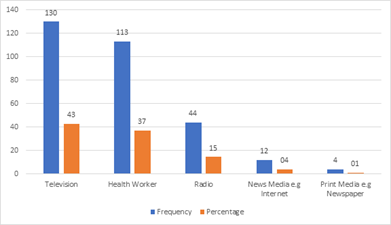
Figure 1: Sources of information on breast cancer among study and control group
The most common source of awareness on breast cancer was television mentioned by 130(43%) of respondents, health worker 113(37%) and radio 44(15%) while the print media accounts for 4(1%).
Table 3: Practice of Breast self-examination by socio-demographic characteristics of respondents
| Factor(s) | Practice | Test statistics (χ2) | p-value | |
| Yes (n=135) | No (n=168) | |||
| Age (years) | 6.889 | 0.076 | ||
| < 30> | 42(31.1) | 72(42.9) | ||
| 30-39 | 77(57.0) | 78(46.4) | ||
| 40-49 | 14(10.4) | 18(10.7) | ||
| ≥ 50 | 2(1.5) | 0 (0.0) | ||
| Marital status | 1.622 | 0.445 | ||
| Single | 2(1.5) | 6(3.5) | ||
| Married | 127(94.1) | 157(93.5) | ||
| Widow | 6(4.4) | 5(3.0) | ||
| Type of marriage | 3.18 | 0.08 | ||
| Monogamy | 132 (97.8) | 157(93.5) | ||
| Polygamy | 3(2.2) | 11(6.5) | ||
| Parity | 5.43 | 0.02* | ||
| < 4> | 59(43.7) | 96(57.1) | ||
| ≥ 4 | 76 (56.3) | 72(42.9) | ||
| Total | 135 | 168 | ||
| Religion | 1.795 | 0.408 | ||
| Christianity | 83(61.5) | 97(57.7) | ||
| Islam | 52(38.5) | 71(42.3) | ||
| Total | 135 | 168 | ||
| Level of Education | 3.313 | 0.517 | ||
| None | 0.0 | 1(0.1) | ||
| Informal | 3(2.2) | 4(2.4) | ||
| Primary | 28(20.7) | 24(14.3) | ||
| Secondary | 98(72.6) | 128(76.2) | ||
| Tertiary | 6(4.4) | 11(6.5) | ||
| Total | 135 | 168 | ||
| Husband’s occupational status | ||||
| Officer | 1(0.8) | 0(0.0) | 6.170 | 0.222 |
| soldier | 129(97.7) | 151(95.0) | ||
| Civil servant | 2(1.5) | 4(2.5) | ||
| Trading | 0(0.0) | 3(1.9) | ||
| Others | 0(0.0) | 1(0.6) | ||
| Total | 132 | 159 | ||
| Occupational Status of woman | 5.074 | 0.165 | ||
| House wife | 96(72.7) | 117(71.8) | ||
| Trading | 19(14.4) | 31(19.0) | ||
| Civil servant | 15(11.4) | 9(5.5) | ||
| Others | 2(1.5) | 6(3.7) | ||
| Total | 132 | 163 | ||
Only parity was found to be associated with practice of breast self-examination as 56.3% of respondents who have had four or more deliveries practice breast self-examination (p=0.02).
Table 4: levels of practice of breast self-examination by awareness and knowledge of women.
| Factor(s) | Practice | Test statistics (χ2) | p-value | |
| Yes | No | |||
| Awareness | 5.622 | 0.018* | ||
| Yes | 123(91.1) 137(82.1) | |||
| No | 12 (8.9) 31(18.5) | |||
| Total | 135 168 | |||
| Knowledge | 8.088 | 0.004* | ||
| Good | 46(34.1) 33(19.6) | |||
| Poor | 89(65.9) 135(80.4) | |||
| Total | 135 168 | |||
P less than 0.05
Majority 123(91.1%) of respondents who were aware of breast cancer practice breast self-examination with a statistically significant difference (p=0.018), while 46(34.1%) of respondents with good knowledge of breast cancer practice breast self-examination, (p=0.004).
Table 5: Factors associated with practice of breast self-examination among respondence
| Factor(s) | P-Value | AOR | 95% Confidence interval |
| Lower-Upper | |||
| Parity | |||
| ≥ 4 | 0.015 | 1.8 | 1.122 -2.888 |
| < 4> | 1 | ||
| Awareness | |||
| Yes | 0.061 | 1.992 | 0.968-4.099 |
| No | 1 | ||
| Knowledge | |||
| Good | 0.005 | 2.162 | 1.263 -3.701 |
| Poor | 1 | ||
| Constant | 0 | 0.269 | |
Parity (p=0.015), and knowledge (p=0.005) remained statistically significant in the multiple logistic models, respondents who are multiparous were 80% more likely to practice breast self-examination than non-multiparous women, also respondents with good knowledge were two times more likely to practice breast self-examination than those with poor knowledge. The confidence intervals for parity and knowledge did not include the null value of one, making it a significant finding
Findings of in-depth interview on breast cancer screening practices known to respondence
Majority of the women do not practice any of the breast cancer screening options (BSE, CBE and mammography), among the few women that practice breast Examination, more women reported practice of BSE than CBE, none reported practice of mammography.
Barriers and /or motivating factors to practice breast examination
All the women agree that their husbands made almost all decisions, more so that the issue at hand is a sensitive reproductive health issue, they will require consent from their husbands to go for CBE and mammography, they will also be more willing to go for CBE if it’s a female doctor or nurse that will be performing the procedure on them, as for BSE, they don’t think there is any barrier, even their husbands can support them while doing it during for-play. Others mentioned cost of transport, time spent at health care centre and attitude of HCW towards them Some of their responses are as follows: “I heard on social media that it helps for a man or husband to touch a woman’s nipple that it helps or protects, but I don’t know how true it is, as for me my husband does not support me in this regard”
Women’s experiences with breast cancer screening practices
The women said they have no experience since they don’t practice breast examination, they are hearing this for the first time, they however agreed it will offer some advantage since it will help identify any breast problem early for the woman to take necessary action needed to prevent it or even identify it at early stage.
Benefits of practicing breast examination
All respondence said they are sure it will help identify any breast problem early for the woman to take necessary action needed to prevent it from getting worst or even identify it at early stage.
Mrs S7 said “I really don’t know, but we will come so that you people (health workers) will teach us, but am sure when you get to identify a problem at its early stage then you save yourself a lot of problem”.
Discussion
The mean age (± SD) of respondents was 32.3±7 with a range of 20 to 54 years, with majority of the respondence in the age bracket of 30 to 39 years, collaborating previous studies [23-26] however in Egypt a lower mean age and range was reported, the difference may be because the latter study was done among university students [27]. Majority of respondence in this study have secondary education, this was higher than findings from Southwest of Nigeria, this may be because the study former studies were done among rural women [23,24].
There was a progressive decline in the awareness of BC, BSE, CBE and mammography respectively, similar to findings from Zaria, Ibadan, Lagos and Benin.1-3,23,24,26 Awareness of breast self-examination was lowest among women less than 30 years, which was a similar finding in other surveys [4,28]. This finding underscores the need for more tailored health education messages not just on breast cancer but also on breast cancer prevention and screening services.
Findings from the qualitative study also collaborated a progressive decline in the awareness of BC, BSE, CBE and mammography as in-depth interviews found awareness of breast cancer to be higher than the prevention and screening services; eight out of ten interviews affirmed that they have heard of breast cancer. For example, one participant said,” Yes, I know what breast cancer is, I heard that one woman where I was staying before had swollen breast and they said it was breast cancer, I also saw a picture in the phone of a woman with breast cancer last year.
Television and health workers followed by radio were the mean source of information on breast cancer among respondence, this was collaborated by an interviewee during the in-depth interviews narrating how she heard of breast cancer on the television, “am aware, I heard of breast cancer while watching television one evening in my house”. This was not the same finding in Egypt where Television and health workers scored low as a source of information [29] this low value in the latter study may be because the researcher included an option of all of the above, which had a higher score, other studies also found radio as the main source of information [8,24] other sources reported by literatures include elders, neighbours, friends and siblings [30] this may be so especially for rural women, these source of information was also reported during the in-depth interviews, especially among respondence who have family members diagnosed of breast cancer. The source of information in a health education programme is important in order to enable the choice of the appropriate medium to reach the right audience, in such a way to guarantee an efficient and effective communication.
Knowledge on breast cancer among respondence was poor. This was the same finding in previous studies [1-5,25-30] and is collaborated by the in-depth interviews as many of the interviewees could not mention some symptoms and signs of breast cancer, they also couldn’t mention the right persons to carry out clinical breast examination and mammography, one respondence was recorded as saying thus: ” I don’t know how I will recognise breast cancer, that is why I asked for the cause of breast cancer, so honestly I don’t know, am just hearing what breast cancer is for the first time”. The implication of poor knowledge is that the women will not be able to recognise early symptoms and signs, therefore they present mostly with late-stage disease and complications, leading to increased morbidity and mortality as well as an increased burden on the already overstretched health care system.
Less than half of the respondence practice breast self-examination, and practice of clinical breast examination was even lower, in addition none of the respondence has had a mammography prior to the survey. This finding necessitates to need for more tailored health education messages to women in the community to take ownership and responsibility for their health by practicing breast cancer prevention and screening via Breast self-examination, clinical breast examination and mammography as may be appropriate.
Limitations
- Practice of breast examination was measured based on reported practice as opposed to observed practice because of the sensitive nature of breast examination.
- Local literature on health intervention studies on preventive services for breast cancer is few (fewer still amongst women in a community).
Conclusion
Prioritisation of Health education intervention programmes and campaigns on breast cancer prevention and control among women of reproductive age group should be welcomed by policy makers and government in order to raise awareness and empower women to take action towards their health and wellbeing.
Recommendations
- Yearly breast cancer awareness campaigns in the month of October as declared by the World Health Organization should be supported and financed by the Nigeria army medical corps, supported and organised by the medical directors of medical centres in all cantonments and military formations, this will serve as a rallying point for women to take up breast cancer screening services, as well as support women with breast cancer disease.
- Access to breast cancer screening services especially mammography should be provided at all medical centres in the military cantonments in Nigeria, these services should be available to all women irrespective of their ability to pay. Appropriate human resource should also be trained to provide these services; this should be the responsibility of Divisional commandants.
References
- Agbo, H. A., Chingle, M. P., Envuladu, E. A., & Zoakah, A. I. (n.d.). Breast self-examination—A necessary preventive tool: Knowledge and practice among students of College of Education Gindiri, Plateau State. Jos Journal of Medicine, 6(1):47–53.
Publisher | Google Scholor - Gwarzo, U. M., Sabitu, K., & Idris, S. H. (2009). Knowledge and practice of breast self-examination among female undergraduate students. Annals of African Medicine, 8(1).
Publisher | Google Scholor - Okobia, M. N., Bunker, C. H., Okonofua, F. E., & Osime, U. (2006). Knowledge, attitude and practice of Nigerian women towards breast cancer: A cross-sectional study. World Journal of Surgical Oncology, 4(11):4–11.
Publisher | Google Scholor - Balogun, M. O., & Owoaje, E. T. (2005). Knowledge and practice of breast self-examination among female traders in Ibadan, Nigeria. Annals of Ibadan Postgraduate Medicine, 3(2):52–56.
Publisher | Google Scholor - Omotara, B., Yahya, S., Amodu, M., & Bimba, J. (2012). Awareness, attitude and prevalence of rural women regarding breast cancer in north east Nigeria. Journal of Community Medicine and Health Education, 2(5):1–4.
Publisher | Google Scholor - Bellgam, H. I., & Buowari, Y. D. (2012). Knowledge, attitude and practice of breast self-examination among women in Rivers State, Nigeria. Nigerian Health Journal, 12(1):16–18.
Publisher | Google Scholor - World Cancer Research Fund International. (2015). Breast cancer statistics.
Publisher | Google Scholor - Afolayan, A., & Olaoye, O. (2012). Breast cancer trends in Nigerian population: An analysis of cancer registry data. International Journal of Life Sciences and Pharma Research, 2(3):29–34.
Publisher | Google Scholor - International Agency for Research on Cancer. (2012). GLOBOCAN database.
Publisher | Google Scholor - Kene, T. S., Odigie, V. I., Yusufu, L. M., Yusuf, B. O., Shehu, S. M., & Kase, J. T. (2010). Pattern of presentation and survival of breast cancer in a teaching hospital in north western Nigeria. Oman Medical Journal, 25:104–107.
Publisher | Google Scholor - Allemani, C., Weir, H. K., Carreira, H., et al. (2015). Global surveillance of cancer survival 1995–2009: Analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries. The Lancet, 8(5):977–1010.
Publisher | Google Scholor - Mabula, J. B., McHembe, M. D., & Chalya, P. L. (2012). Stage at diagnosis, clinicopathological and treatment patterns of breast cancer at Bugando Medical Centre in north-western Tanzania. Journal of Health Research, 1(4):269–279.
Publisher | Google Scholor - Okobia, M. N., & Osime, U. (2004). Clinicopathological study of carcinoma of the breast in Benin City. African Journal of Reproductive Health, 5:56–62.
Publisher | Google Scholor - Pearson, J. B. (1963). Carcinoma of the breast in Nigeria: A review of 100 patients. British Journal of Cancer Research, 17:559–565.
Publisher | Google Scholor - Winters, Z., Mannell, A., & Esser, J. D. (n.d.). Breast cancer in Black South Africans. South African Journal of Surgery, 26:69–70.
Publisher | Google Scholor - Gebremedhin, A., & Shamebo, M. (1998). Clinical profile of Ethiopian patients with breast cancer. East African Medical Journal, 75:640–643.
Publisher | Google Scholor - Basro, S., & Elstaedt, J. P. A. (2010). Breast cancer in young women in a limited-resource environment. World Journal of Surgery, 34(5):1427–1433.
Publisher | Google Scholor - Ntekim, A., Nufu, F. T., & Campbell, O. B. (2009). Breast cancer in young women in Ibadan, Nigeria. African Health Sciences, 9:242–246.
Publisher | Google Scholor - Anyanwu, S. N. (2000). Survival following treatment of primary breast cancer in eastern Nigeria. East African Medical Journal, 77:539–543.
Publisher | Google Scholor - Ezeome, E. R. (2010). Delays in presentation and treatment of breast cancer in Enugu, Nigeria. Nigerian Journal of Clinical Practice, 13(3):311–316.
Publisher | Google Scholor - Mark, M. (2010). Sample size and saturation in PhD studies using qualitative interviews. Journal of Qualitative Social Research, 11(3):8.
Publisher | Google Scholor - Araoye, M. O. (2004). Research methodology with statistics for health and social sciences (123–127).
Publisher | Google Scholor - Amoran, O. E., Toyobo, T. O., & Fatugase, O. K. (2014). Breast cancer screening awareness and practice among women in Sagamu Local Government Area, South-Western Nigeria: A community-based study. British Journal of Applied Science & Technology, 4(16):20–24.
Publisher | Google Scholor - Ajayi, I. O., Onibokun, A. C., & Soyannwo, O. A. (2013). Breast and cervical cancer awareness and screening practices among rural women in Ona-Ara Local Government Area, Ibadan. African Journal of Biomedical Research, 16(1):95–99.
Publisher | Google Scholor - Ogunbode, A. M., Fatiregun, A. A., Ogunbode, O. O., & Adebusoye, L. A. (2013). Breast examination as a cost-effective screening tool in a clinical practice setting in Ibadan, Nigeria. African Journal of Primary Health Care & Family Medicine, 5(1):7–14.
Publisher | Google Scholor - Obaji, N. C., Elom, H. A., Agwu, U. M., Nwigwe, C. G., Ezeonu, P. O., & Umeora, O. U. J. (2013). Awareness and practice of breast self-examination among market women in Abakaliki, South East Nigeria. Annals of Medical and Health Sciences Research, 3(1):7–12.
Publisher | Google Scholor - Mohammad, F. A., & Mohammed, M. (2013). Efficacy of instructional training program in breast self-examination and breast screening for cancer among university students. Public Health Research, 3(3):71–78.
Publisher | Google Scholor - Isara, A. R., & Ojedokun, C. I. (2011). Knowledge of breast cancer and practice of breast self-examination among female senior secondary school students in Abuja, Nigeria. Journal of Preventive Medicine and Hygiene, 4(2):52–54.
Publisher | Google Scholor - Seham, A., Abd, E. H., & Nabila, S. M. (2015). Effect of educational program about breast cancer knowledge and breast self-examination training on building accurate information and behavior among women. Journal of Natural Science Research, 5(4):58–70.
Publisher | Google Scholor - Oluwatosin, O. O., & Oladepo, O. (2006). Knowledge of breast cancer and its early detection measures among rural women in Akinyele Local Government Area, Ibadan, Nigeria. BMC Journal, 6(2):27–33.
Publisher | Google Scholor























